# Indications For Echo in Hypertension 高血压患者的超声适应症
- Second line assessment ESC Guidance 2013 “the routine use of echo in systemic hypertension is inappropriate"
在系统性高血压中常规使用超声是不合适的 - Assess if there is end organ damage
评估是否存在终末器官损害- Grade 1 hypertension to decide on Rx
- Cardiovascular risk
- 血压越高,心脑血管疾病风险越高[1]
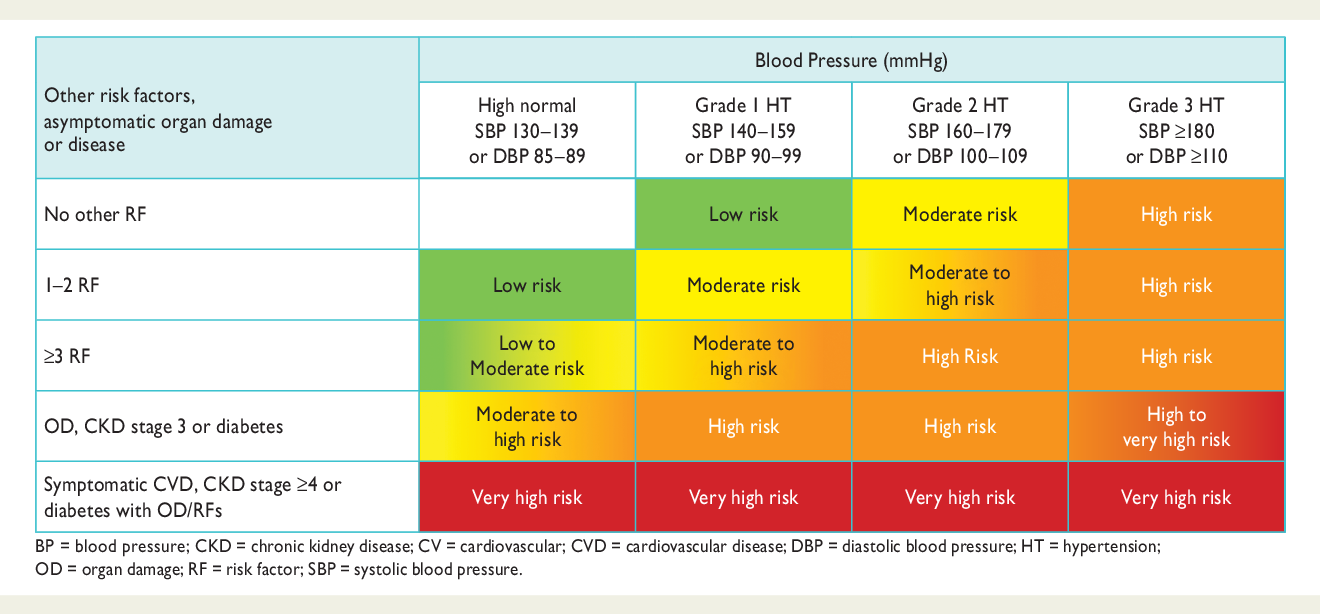
- Stratification of total CV risk in categories of low, moderate, high and very high risk according to SBP and DBP and prevalence of RFs, asymptomaticOD, diabetes,CKDstageor symptomaticCVD. Subjects with ahigh normaloffice but a raisedout-of-office BP (maskedhypertension) have a CV risk in the hypertension range. Subjects with a high office BP but normal out-of-office BP (white-coat hypertension), particularly if there is no diabetes, OD, CVD or CKD, have lower risk than sustained hypertension for the same office BP. [2]
- Asymptomatic 无症状的
- OD: organ damage 器官损伤
- CKD: chronic kidney disease 慢性肾病
- CVD: cardiovascular disease 心血管疾病


Assess for LV failure if suspect heart failure(symptoms, signs, abnormal ECG, abnormal CXR).
如果怀疑心力衰竭 (症状、体征、异常的心电图、异常的胸片 chest x-rays),评估是否有左心衰竭。Suspicion of structural heart disease
怀疑有结构性心脏病- Symptoms
- Murmur 杂音
- Suspect Coarctation 可疑狭窄
- Coarctation of the aorta, CoA 主动脉狭窄
Suspicion for CAD - anginal/abnormal ECG.
怀疑为冠心病 - 心绞痛 / 异常心电图。
# Hypertension Heart Disease
- Coronary Artery Disease, CAD 冠状动脉疾病
- Heart Failure 心力衰竭
- Diastolic Dysfunction 舒张功能障碍
- Impaired relaxation 松弛功能受损
- Left ventricular myocvte hypertrophy 左心室肥厚
- Interstitial fibrosis 间质纤维化
- Systolic Dysfunction 收缩功能障碍
- Ischaemic cardiomyopathy 缺血性心肌病
- Late consequence of afterload 后负荷的后期后果
- Diastolic Dysfunction 舒张功能障碍
- Arrhythmias 心律失常
- Atrial fibrillation 心房颤动
- Left atrial enlargement 左房增大
- Ventricular Arrhythmias 室性心律失常
- Atrial fibrillation 心房颤动
# Left Ventricular Hypertrophy (LVH) 左室肥厚
高血压导致心脏压力负荷过高,可导致左室肥厚;血压控制后,左室肥厚可能减轻
Effect of mechanical loading most clear in rapid regression following aortic valve replacement
主动脉瓣狭窄也会导致左室肥厚,主动脉瓣置换后压力负荷降低后,左室肥厚的程度有所缓解In systemic hypertension confounded by role of angiotensin II and sympathetic hormones
血管紧张素 II 和交感神经激素在高血压中的作用LVH often develops after other signs of diastolic dysfunction in HTN
左室肥厚出现在舒张期功能障碍症状出现后LVH also seen to precede development of systemic HTN.
也有部分患者的左心室肥厚先于系统性高血压发生。- 如果患者出现心电图或者心超的改变,需要关注 LVH 和高血压的情况
Concentric increase in LV mass
左心室质量向心性增大Compensatory response to increased afterload
对后负荷增加的补偿反应Collagen
胶原Myocyte hypertrophy
肌细胞肥厚
# Consequences of LVH 后果
- Initially compensatory, ultimately associated with risk of cardiovascular events
最初是代偿性的,最终与心血管事件的风险有关 - Ischaemia 缺血
- Decreased coronary reserve with increased LV mass
随着左室质量增加,冠状动脉储备减少- Angina 心绞痛
- Greater risk of death following myocardial infarction
心肌梗死后死亡风险增大
- Decreased coronary reserve with increased LV mass
- Heart Failure 心力衰竭
- Depressed LV systolic and diastolic function
左室收缩和舒张功能降低
- Depressed LV systolic and diastolic function
- Arrhythmia 心律失常
- Atrial fibrillation 心房颤动
- Ventricular arrhythmias 室性心律失常
- Non-uniform action potential prolongation
非均匀动作电位延长 - Altered repolarization
复极化改变 - Specific vulnerability to torsade
- Ischaemic ventricular arrhythmia
缺血性室性心律失常
- Non-uniform action potential prolongation
# Patterns of Left Ventricular Hypertrophy 左室肥厚的类型
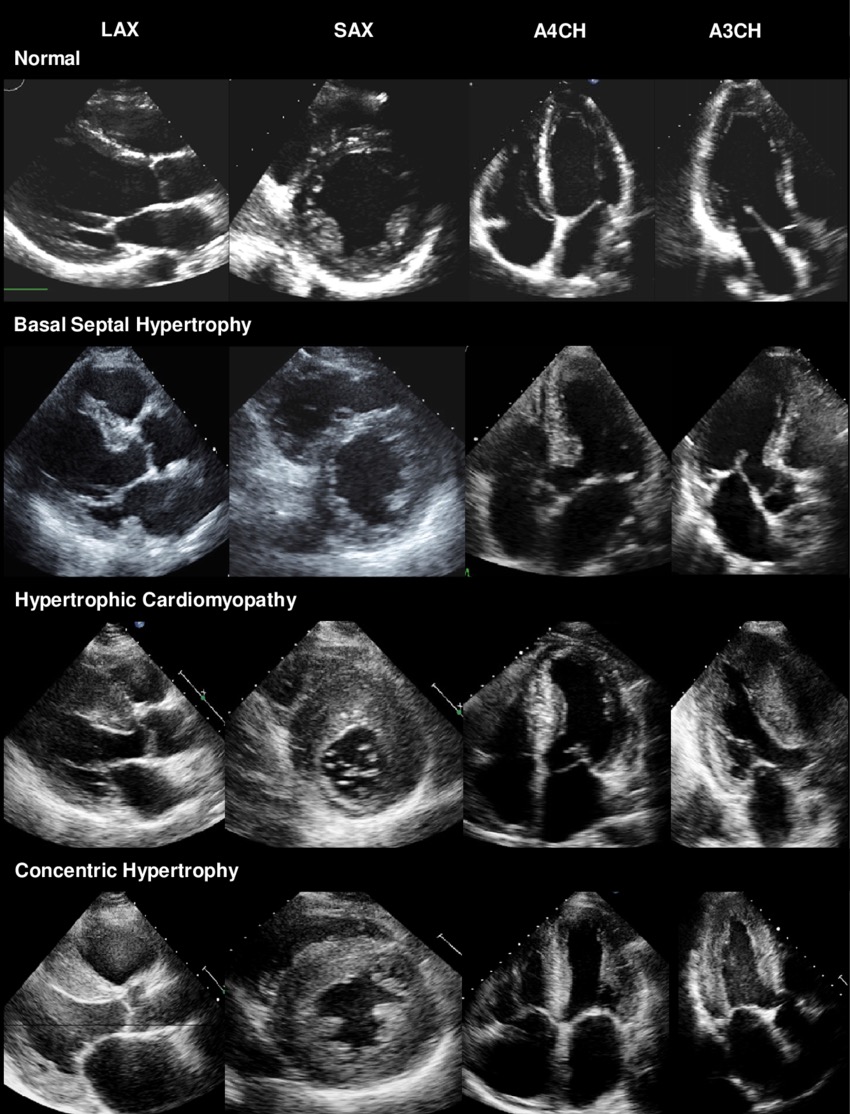
- Comparison of normal myocardium, basal septal hypertrophy(BSH), HCM, and concentric LVH on conventional two-dimensional echocardiography. PLAX = parasternal long axis view, SAX = short axis view, A4CH = apical 4-chamber view, A3CH= apical 3-chamber view. [3]
- 正常室壁
- 间隔基底段肥厚,从 PLAX、A4C、A3C 可以看到仅是基底段的肥厚,SAX 在容积水平的室壁厚度是正常的
- 肥厚型心肌病(不对称性肥厚),SAX 可以看到前壁、前侧壁呈现明显的心肌肥厚,下壁和下侧壁的厚度是正常的
- 向心性肥厚(高血压患者常见),如果室壁肥厚超过 15 mm 则倾向于认为是遗传性的肥厚而非高血压继发的
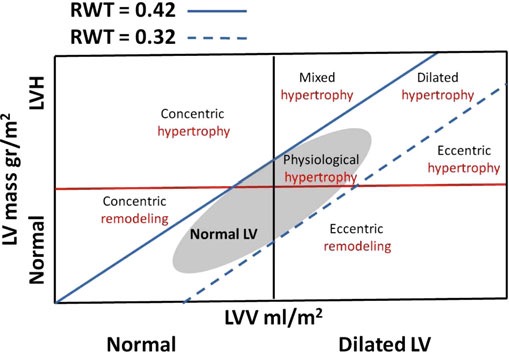
- LV geometric patterns classified according to LVM, LV volume, and RWT. [4]
LV 几何形态按 LVM、LV 体积和 RWT 分类。- The red horizontal line separates LVH from normal LVM. The black vertical line separates dilated from nondilated ventricles. The two oblique blue lines delimit the upper (0.42) and lower (0.32) limit of normal RWT. This leads to eight categories of ventricles. The grey ellipse indicates the area of normal ventricles including physiological LV enlargement.
红色水平线将 LVH 与正常 LVM 分开。黑色垂直线将扩张的心室与非扩张的心室分隔开来。两条蓝色斜线划定了正常 RWT 的上限(0.42)和下限(0.32)。这分成了八种类型的心室。灰色椭圆表示正常心室的面积,包括生理性 LV 增大。 - LVM: left ventricular (LV) mass 左室质量
- RMW: the ratio of twice the posterior wall
thickness (PW) and the LV diastolic diameter
后壁厚度 (PW) 的两倍与左心室舒张期内径之比
- The red horizontal line separates LVH from normal LVM. The black vertical line separates dilated from nondilated ventricles. The two oblique blue lines delimit the upper (0.42) and lower (0.32) limit of normal RWT. This leads to eight categories of ventricles. The grey ellipse indicates the area of normal ventricles including physiological LV enlargement.
# Compare Physiology from Pathology 生理性肥厚与病理性肥厚对比
| HYPERTENSIVE HEART | ATHLETES | |
|---|---|---|
LV wall thickness | Increased | Increased |
LV diastolic dimension | Decreased, N, or increased | Increased |
LV systolic dimension | Decreased, N, or increased | Increased |
Stroke volume | Increased | Increased |
Fractional shortening | High, N, or depressed | Preserved |
Diastolic dysfunction | Often present | Absent |
LV wall strain | Present | Absent |
Heart rate | Not affected | Bradycardia |
# Basal Septal Hypertrophy 室间隔基底部肥厚
- 4104 patients in a non-specialised community echo clinic [5]
4104 患者在非专业社区超声诊所 - Retrospective study 回顾性研究
- Prevalence of IBSH was 5.8% (240/4104)
IBSH 患病率为 5.8% - Mean (SD) age was 76.0y (10.4);increased with age
平均 (标准差 standard deviation) 年龄为 76.0 岁 (10.4);随年龄增长而增加 - Equal gender distribution.
性别分布均衡
# 超声表现
- Resting peak LVOT gradient (>20 mmHg) was present in 8/240(3.3%), mean (SD) 69.6mmHg(59.3)
部分基底部肥厚的患者,静息时左室流出道峰值压力梯度 (>20 mmHg) 存在于 8/240 (3.3%),平均 (SD) 69.6mmHg (59.3) - Patients with LVOTO had hyper-contractile LV function(fractional shortening [SD] 51.8% [9.5] vs. 40.5% [10.9], p = 0.012) compared to those without LVOTO
与没有左室流出道梗阻的患者相比,LVOTO 患者的左室功能亢进 (分数缩短 [SD] 51.8% [9.5] vs. 40.5% [10.9],p = 0.012) - Similar BS thickness [SD] (17.8mm [3.0] vs. 17.8 mm [2.8], p =0.996) and ECG characteristics
相似的室间隔基底部厚度 [SD](17.8mm [3.0] vs. 17.8 mm [2.8], p =0.996) 和心电图特征 - Greater apical and septal displacements of the mitral valve coaptation point characterized those with LVOTO.
LVOTO 患者的特征是其二尖瓣对合处,有较大的心尖和室间隔的移位。
# WHY does BSH occur? 为什么 BSH 会发生
- Not well understood 不是很明确
- Link to hypertension especially in elderly females. 与高血压有相关性,而且表现为这个老年女性居多
- Largest radius thus highest wall force (Laplace's law)
根据拉普拉斯定律,半径越大,对壁的作用力越大 - Last part of the LV to be activated-hence contracts against highest pressure
左室的基底段是最后一处被激活的用于对抗高血压的地方,所以它就会呈现局部增厚 - Interaction with RV contraction
也有可能与右室收缩有相互作用的关系
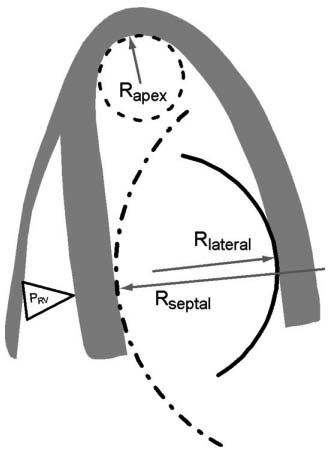
- Non-uniformity of the LV (longitudinal) curvature. [6]
LV (纵向) 曲率不均匀- R apex : radius of curvature at the apex;
心尖的曲率半径 - R lateral : radius of curvature at the lateral wall;
侧壁的曲率半径 - R septal : radius of curvature of the septum;
室间隔的曲率半径; - PRV: pressure in the right ventricle.
右室的压力
- R apex : radius of curvature at the apex;
# ECG in Evaluation of LVH 心电图评价左室肥厚
- The ECG is valuable for detection of LVH, at least in patients over 55 years
心电图对检测 LVH 很有价值,至少在 55 岁以上的患者中是如此 - Electrocardiography can also be used to detect patterns of ventricular overload or 'strain' suggesting more severe risk, ischaemia, conduction abnormalities, left atrial dilatation
心电图也可以用来检测心脏超负荷或 “劳损” 的模式,提示更严重的风险、缺血、传导异常、左房扩张 - Detection of arrhythmias including atrial firillation
检测包括房颤在内的心律失常
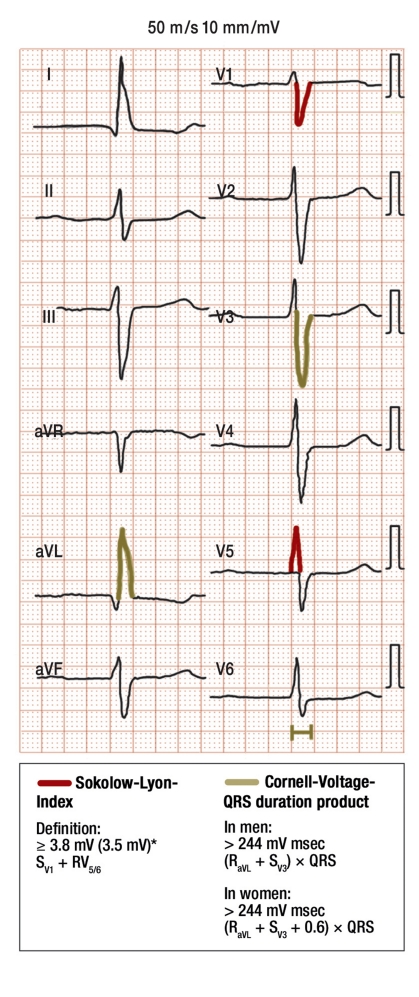
ECG for the diagnostic evaluation of left ventricular hypertrophy [7]
心电图对左室肥厚的诊断价值Sokolow-Lyon index :
Cornell Voltage Product: Cornell 电压积
- Men:
- Women:
- Men:
以及 ST 段压低及 t 波改变
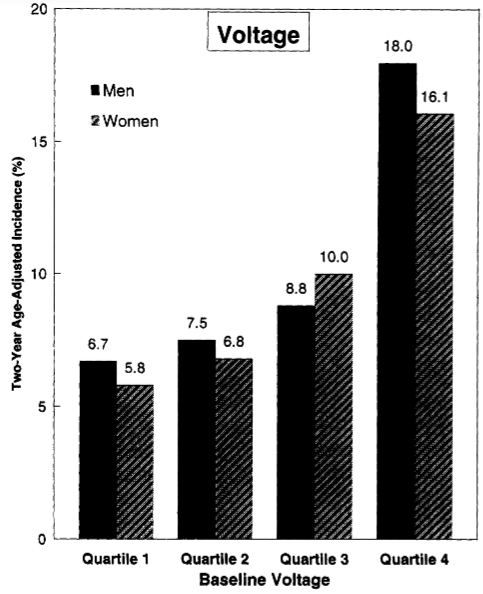
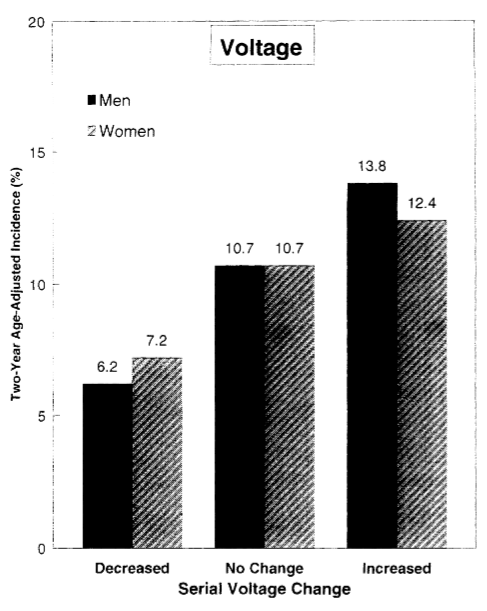
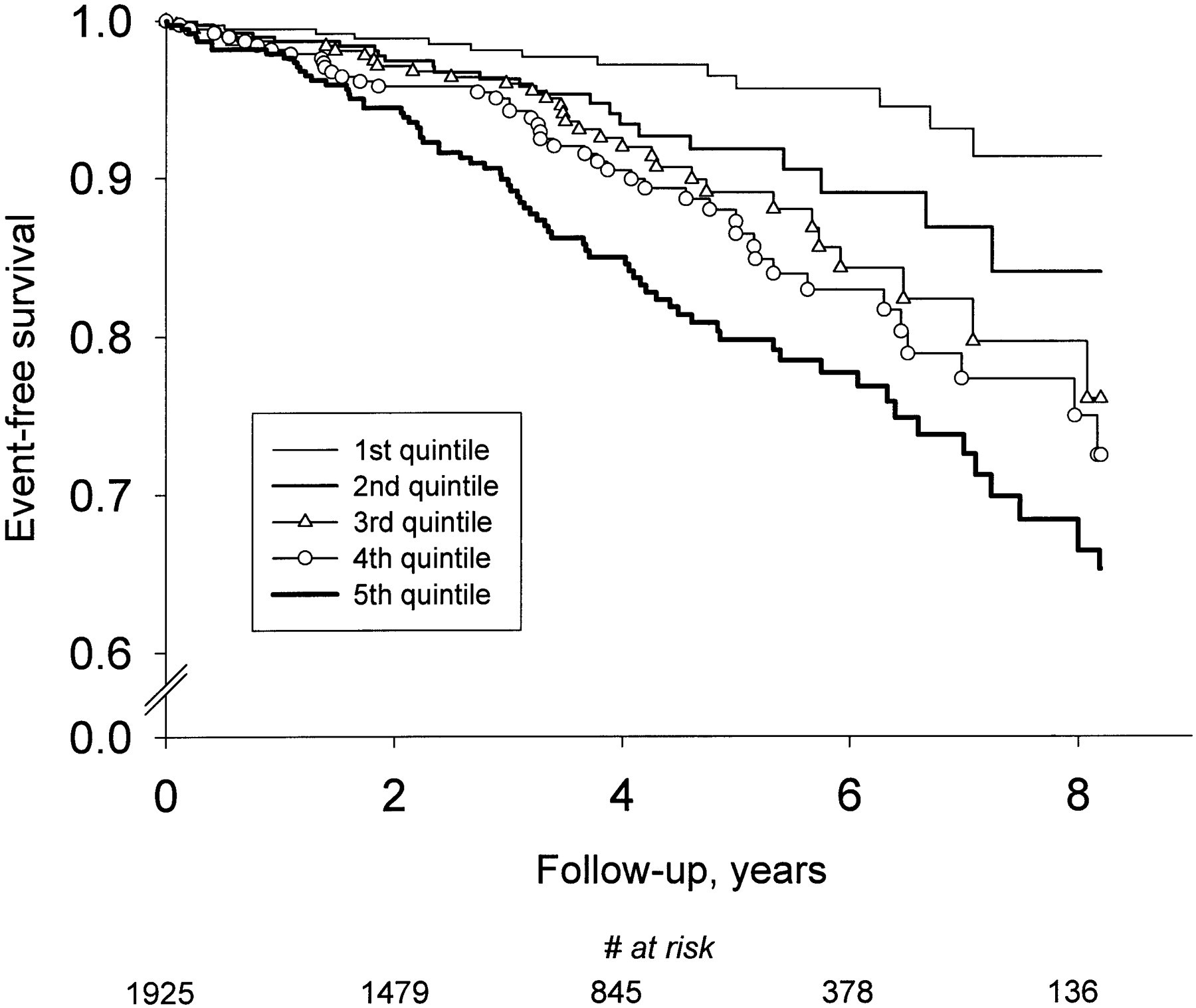
ECG Voltage Criteria and CV Events 心电图电压标准和心血管事件 [8]
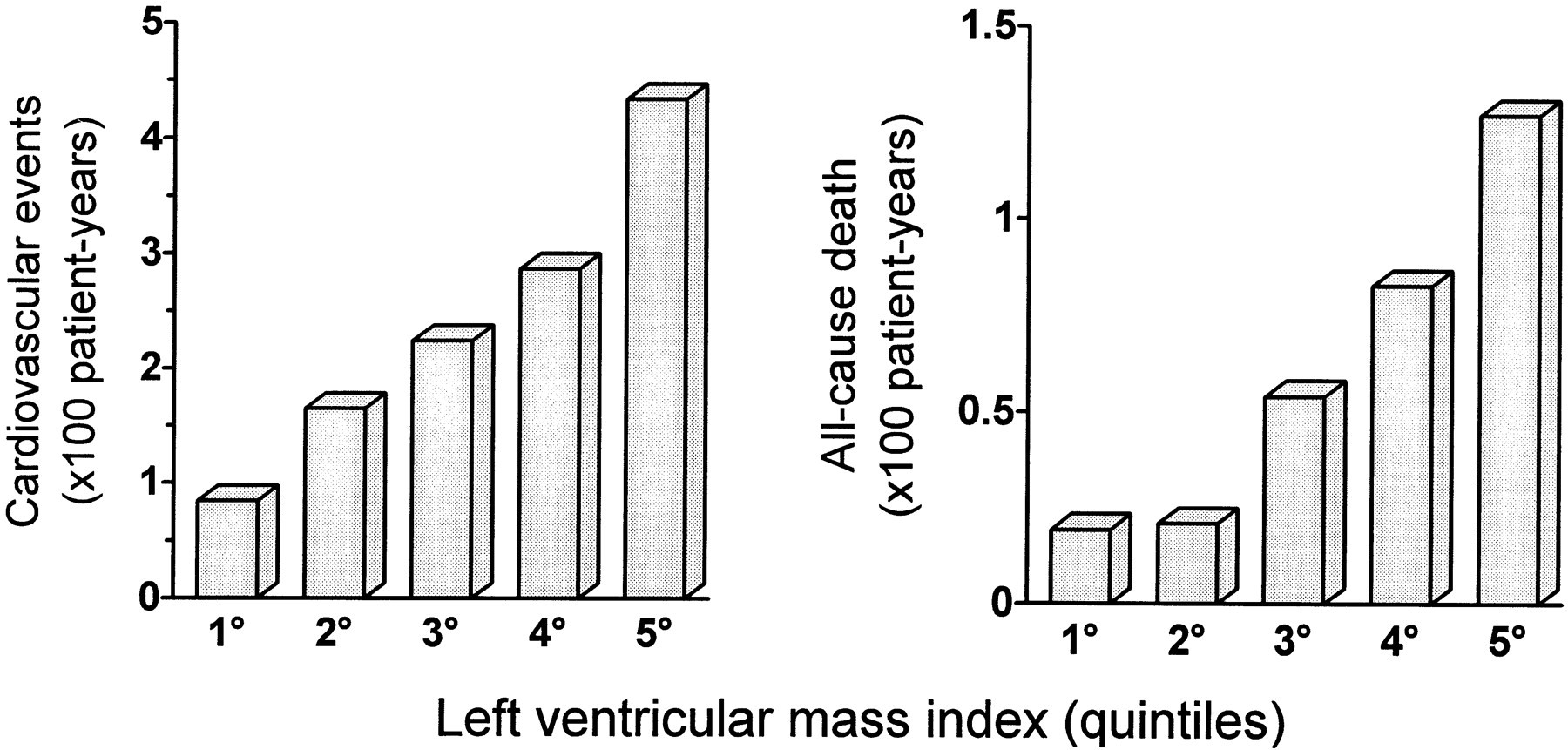
- Left Ventricular Mass and CV Events 左室质量和心血管事件 [9]
# Echocardiography Findings in Systemic HTN 全身性高血压的超声心动图检查结果
- Symmetric left ventricular hypertrophy
对称性左心室肥厚 - Left atrial enlargement
左房增大 - Mitral annular calcification
二尖瓣环钙化- Mild to moderate mitral regurgitation
轻度至中度二尖瓣反流
- Mild to moderate mitral regurgitation
- Aortic root dilatation
主动脉根部扩张 - Aortic valve sclerosis
主动脉瓣硬化- Mild aortic regurgitation
轻度主动脉瓣反流
- Mild aortic regurgitation
- Diastolic dysfunction
舒张功能障碍- Impaired relaxation
松弛受损 - Restrictive pattern
限制性模式
- Impaired relaxation
- Reduced ejection fraction
射血分数降低- Usually late consequence with ventricular dilatation
通常是心室扩张的晚期后果
- Usually late consequence with ventricular dilatation
# Echocardiographic Evaluation of LVH
- Framingham adds echocardiography in 1979
- ECG probably has 1/8th the sensitivity of echocardiography
心电图对 LVH 的敏感度可能只有超声心动图的 1/8- Probably 20 percent prevalence in those over 40 years old
在 40 岁以上的人群中可能有 20% 的发病率- Present in 20 to 30 percent of otherwise low risk patients with HTN.
存在于 20% 至 30% 的其他低风险的高血压患者中。
- Septal/PW thickness 室间隔 / 后壁的厚度
- LV mass 左室质量
- 测量方法有很多
- CUBE FORMULA 立方体公式
- LV mass index 左室质量指数
- Relative wall thickness 相对室壁厚度
- 2 x PW thickness/LVIDD
- > 0.42 eccentric
# Left Ventricular Mass Calculation
临床上左室质量的测量方法有 M 型二维、三维超声心动图,运用的原理基本都是左室心外膜包含的体积减去左室室腔的体积,得到心外膜和心腔之间左室心肌的体积,再乘以心肌的密度。
立方体公式:当胸骨旁长轴测量了室间隔的厚度、左室舒张末期的内径以及下侧壁的厚度,系统会自动给出左室的质量。但每个仪器假设左室的几何形态的不同,运用的公式也略有不同,但是原理都是相似的,系统会给出患者左室质量的绝对值。
目前临床上运用最多的是左室质量指数,包括对体表面积的指数,以及对身高的指数,这样才能对每个个体患者的左室质量进行一个相对比较准确的评估,看有没有左室肥厚。
Echocardiographic Criteria for Normal Upper Limits of LV Mass [10] | ||
|---|---|---|
| Men | Women | |
| n | 347 | 517 |
| Age, y | 42±12 | 43±12 |
| LV mass, absolute, g | 259 | 166 |
| LV mass, corrected for BSA, g/m2 | 131 | 100 |
| LV mass, corrected for height, g/m | 143 | 102 |
BSA indicates body surface area. 体表面积
Left ventricular mass and left ventricular mass indexed to body surface area estimated by LV cavity dimension and wall thickness at end-diastole.
左心室质量和左心室质量与体表面积相关,由舒张末期的 LV 腔尺寸和壁厚估计。Advantages 优势
- Fast/widely used
快速 / 广泛使用 - Supported by published data with prognostic value
已发布大量有预测价值的数据支持 - Fairly accurate with normal LV shape e.g. for concentric LVH
对于正常 LV 形状,相当准确,例如向心性 LVH - Good for screening large populations.
适合筛查大量人群
- Fast/widely used
Disadvantages 劣势
- Based on shape assumptions (2:1 long-short axis ellipsoid with symmetrical LVH)
方法依赖于对几何形状的假设(长短径 2:1 的椭圆体的对称的 LVH,如果实际形状越偏离这样的假设,则测量结果误差越大) - Beam orientation axis errors magnified as measurements are cubed.
超声束方向轴的误差随着测量计算时的立方而放大。
- Based on shape assumptions (2:1 long-short axis ellipsoid with symmetrical LVH)
# Relative wall thickness 相对室壁厚度
- Relative wall thickness (RWT) allows further classification of LV mass increase as either concentric hypertrophy (RWT > 0.42) or eccentric hypertrophy (RWT ≤ 0.42).
相对壁厚(RWT)可以进一步将左室质量增加分为向心性肥厚(RWT > 0.42)或偏心性肥厚(RWT ≤ 0.42)
# 3D echo 三维超声心动图
Advantages 优点
- More precise measurement of LV mass without assumption of LV shape and hypertrophy pattern
更精确地测量 LV 质量,无需假设 LV 形状和肥大模式 - Excellent correlation to CMR (better than 2D or M mode)
与 CMR 的良好相关性(优于 2D 或 M 模式) - As automated less inter-observer variability
由于自动化较少观察者间的可变性 - Good for longitudinal follow up of individual patients
有利于个体患者的纵向随访 - Assess for LVEF
评估 LVEF
- More precise measurement of LV mass without assumption of LV shape and hypertrophy pattern
Disadvantages 缺点
- Need good endocardial definition
需要良好的三维超声心动图 - Normal values less well established.
正常值不太确定
- Need good endocardial definition
# LA enlargement 左房扩大
- 20% of hypertensive patients
20% 的高血压患者 - Marker for LA pressure (LV diastolic function)
LA 压力标记(LV 舒张功能) - Predictor for PAF/AF
预测阵发性心房颤动 paroxysmal atrial fibrillation/AF - Measure at end systole PS LA
在收缩末期测量 - Long axis or M Mode short axis
LA 长轴或 M 模式短轴 - Also LA volume corrected for BSA in 4/2 C view.
在 4/2C 切面中使用 BSA 校正 LA 体积
# LA size Area Method 左房大小面积测量方法
- 2c and 4c views at end systole: frame just prior to mitral valve opening
收缩末期的 2c 和 4c 切面:二尖瓣打开前的帧 - Trace inner border of the LA
追踪 LA 的内边界 - Measure from MV insertions- exclude the area under the mitral leaflets and also the LAA and visible pulmonary veins.
从二尖瓣瓣叶附着点开始测量,排除二尖瓣瓣叶下的小三角形的区域,以及左心耳和可见的肺静脉。
# Volumetric disc summation
描绘面积后,计算圆盘容积
- 2c and 4c views at end systole: frame just prior to mitral valve opening
收缩末期的 2c 和 4c 切面:二尖瓣打开前的框架 - Trace inner border of the LA
追踪 LA 的内边界 - Measure from MV insertions- exclude the area under the mitral leaflets (connect the insertions with a straight line) and also the LAA and pulmonary veins
从二尖瓣瓣叶附着点开始测量,排除二尖瓣瓣叶下的区域 (用直线连接附着处) 以及左心耳和肺静脉 - Perform biplane measurement and take mean.
进行双平面测量,取平均值。
# LA function 左房功能
包括:
- Reservoir - Early diastole
储存,舒张早期 - Conduit - Mitral opening
通道,二尖瓣开口 - Atrial Booster - Late diastole atrial contraction
泵功能,舒张晚期心房收缩
- Reservoir - Early diastole
Accurate assessment of LA function remains cumbersome
LA 功能的准确评估仍然很麻烦LA EF requires a skilful acquisition technique and calculations that are not routinely performed
LA EF 需要熟练的采集技术和计算,而这些技术和计算不是常规执行的The newer parameters assessed by TDI/STE are reproducible and probably more sensitive than traditional ones
TDI, tissue Doppler imaging 组织多普勒成像 / STE, speckle tracking ECHO 斑点追踪超声心动图,评估的新参数是可重复的,并且可能比传统参数更敏感A thorough evaluation of atrial function may assist in the early detection of "subclinical disease" could refine risk stratification, could guide therapy
对心房功能的全面评估可能有助于早期发现 “亚临床疾病”,可以完善风险分层,可以指导治疗The extent of reversibility of LA remodelling with medical therapy, and the impact of such changes on outcomes need further studies.
药物治疗对 LA 重塑的可逆性程度,以及此变化对结果的影响需要进一步研究。
# Diastolic Dysfunction 舒张功能
Patterns of Left Ventricular Diastolic Filling as Shown by Standard Doppler Echocardiography. [11]
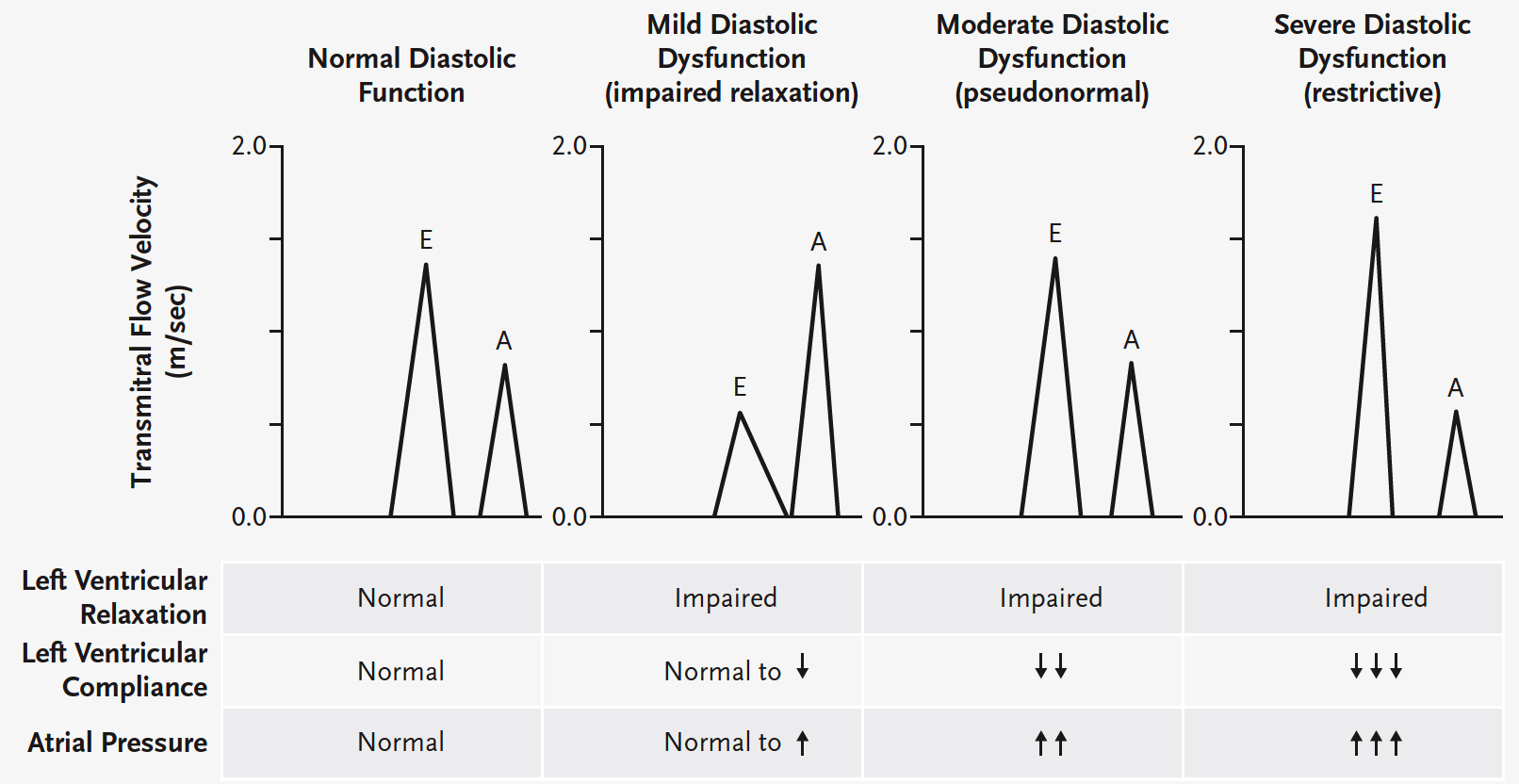
Normal diastolic function | Mild diastolic dysfunction | Moderate diastolic dysfunction | Severe diastolic dysfunction | |
|---|---|---|---|---|
| LV relaxation 左室松弛 | 正常 | 受损 | 受损 | 受损 |
| LV compliance 左室顺应性 | 正常 | 正常或↓ | ↓↓ | ↓↓↓ |
| Atrial pressure 房压 | 正常 | 正常或↑ | ↑↑ | ↑↑↑ |
# Systolic Dysfunction 收缩功能
If regional abnormality consider additional IHD diagnosis
如果局部异常,考虑额外的 IHD 诊断Last stage of hypertensive heart disease 高血压性心脏病末期
- LVEF - Most commonly used index (Simpson's)
LVEF - 最常用的指数 (辛普森指数)
- LVEF - Most commonly used index (Simpson's)
LV long axis function occurs at early stage
LV 长轴功能发生在早期- TDI
- Strain imaging (speckle tracking) - Less operator error (correlates with serum MMP1 - marker of tissue fibrosis);
应变成像(斑点追踪)- 更少的操作失误(与血清 MMP1 相关 - 组织纤维化标志物)- GLS and regional strain patterns
global longitudinal strain 整体长轴应变 和 节段应变
- GLS and regional strain patterns
Finally LV dilatation and reduced EF if left untreated.
如果不及时治疗,可导致左室扩张并出现 EF 降低
| Parameter | Abnormal if [12] |
|---|---|
| LV mass index (g/m2) | > 95 (women) |
| >115 (men) | |
| Relative wall thickness (RWT) | > 0.42 |
| Diastolic function: | |
| Septal e' velocity (cm/sec) | < 8 |
| Lateral e' velocity (cm/sec) | < 10 |
| LA volume index (mL/m2) | ≥ 34 |
| LV Filling pressures: | |
| E/e' (averaged) ratio | ≥ 13 |
# Aortopathy 主动脉病变
Aortic root dilatation 主动脉根部扩张
Also affects aorta at all levels 也会影响所有水平的大动脉
Associated aortic sclerotic change 主动脉的硬化改变
Hence, mild AR is common.
轻度主动脉瓣返流很常见在三个水平进行测量
- Sinuses of Valsalva 乏氏窦
- Sino-tubular junction 窦管交界
- Ascending aorta 升主动脉
- Leading edge to leading edge
前缘到前缘 - Use Zoom mode on PTLAX 2D view
- Measure at end-diastole except for annulus (virtual annulus measured in mid- systole).
除瓣环外,在舒张末期测量 (在收缩中期测量的虚拟瓣环)。
JBS 2: Joint British Societies' guidelines on prevention of cardiovascular disease in clinical practiceHeart 2005;91:v1-v52. ↩︎
Mancia, Giuseppe et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). European heart journal 34 28 (2013): 2159-219 . ↩︎
Kelshiker, Mihir & Mayet, Jamil & Unsworth, Beth & Okonko, Darlington. (2013). Basal Septal Hypertrophy. Current cardiology reviews. 9(4). ↩︎
Marwick, T. H. et al. Recommendations on the use of echocardiography in adult hypertension: a report from the European Association of Cardiovascular Imaging (EACVI) and the American Society of Echocardiography (ASE)†. Eur Heart J Cardiovasc Imaging 16, 577–605 (2015). ↩︎
Ranasinghe, I., Ayoub, C., Cheruvu, C., Freedman, S. B. & Yiannikas, J. Isolated hypertrophy of the basal ventricular septum: Characteristics of patients with and without outflow tract obstruction. International Journal of Cardiology 173, 487–493 (2014). ↩︎
Baltabaeva, A. et al. Regional left ventricular deformation and geometry analysis provides insights in myocardial remodelling in mild to moderate hypertension. Eur J Echocardiogr 9, 501–508 (2008). ↩︎
Schmieder R. E. (2010). End organ damage in hypertension. Deutsches Arzteblatt international, 107(49), 866–873. ↩︎
Levy D, Salomon M, D'Agostino R B, et al. Prognostic implications of baseline electrocardiographic features and their serial changes in subjects with left ventricular hypertrophy[J]. Circulation, 1994, 90(4): 1786-1793. ↩︎
Schillaci G, Verdecchia P, Porcellati C, et al. Continuous relation between left ventricular mass and cardiovascular risk in essential hypertension[J]. Hypertension, 2000, 35(2): 580-586. ↩︎
Lorell B H, Carabello B A. Left ventricular hypertrophy: pathogenesis, detection, and prognosis[J]. Circulation, 2000, 102(4): 470-479. ↩︎
Aurigemma, G. P. & Gaasch, W. H. Diastolic Heart Failure. New England Journal of Medicine 351, 1097–1105 (2004). ↩︎
Mancia, G. et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 31, 1281–1357 (2013). ↩︎