# Learning Objectives
- RV anatomy, haemodynamics and contractility
右室解剖、血流动力学和收缩性能 - Ventricular interdependence
心室相互依赖 - Basic views of the RV
右室的基本切面 - Dimensions and thickness of the RV
右室的尺寸和厚度 - Assessing RV function - tricuspid annular plane systolic excursion(TAPSE), fraction area change(FAC), tissue Doppler imagings(TDI) S' and Tei index
评估右室功能 - 三尖瓣环平面收缩期偏移、面积变化分数、组织多普勒成像和心肌做功指数 - Assessing RV systolic pressure
评估右室收缩压,从而评估肺动脉的压力 - RV strain - not routine
了解右室应变 - 不是常规 - Limitations of RV function assessments
右室功能评估的局限性
# RV anatomy, haemodynamics and contractility
# Right Ventricle Anatomy 右室解剖
- Anterior to the LV and posterior to the sternum
右室位于左室前面和胸骨后面 - Thin walled and compliant chamber
室壁薄,心腔顺应性强 - Asymmetrical and crescent shaped
不对称和新月形 - Divided into inflow tract, infundibulum (outflow) and the apex
分为流入道、漏斗部(流出道)和布满肌小梁的心尖部 - Three muscular bands: Parietal, septomarginal and the moderator band.
解剖学上可以看到三种肌束:位于腔壁的、隔缘的和隔缘肉柱(节制带)。
# RV Coronary Supply 右室冠脉血供
- Coronary flow maintained throughout cycle due to low intraventricular pressure
由于右心室内压低,冠状动脉血流在整个心动周期内都保持 - Hence effect of decreased diastolic perfusion in tachycardia does not affect RV perfusion as much as it affects the LV
因此,心动过速时,舒张期冠脉灌注降低的影响对右室灌注的影响不如对左室的影响大 - RV free wall and posterior third of septum - supplied by the RCA
RV 游离壁和后三分之一的间隔 - 由 RCA 供血 - Apex and anterior 2/3 of septum - supplied by LAD.
心尖部和前 2/3 的间隔 - 由 LAD 供血
# RV Contractility 右室收缩能力
- RV contraction is 'peristaltic'
右室收缩呈 “蠕动” 的形态 - Predominantly longitudinal muscle fibres
主要是纵向肌肉纤维 - Three different mechanisms:
右室收缩三种不同的机制:- Inward movement of the free wall
游离壁的向内移动 - Contraction of longitudinal fibres
纵向纤维的收缩 - Traction of the free wall at points of attachment secondary to LV contraction
左室收缩后,附着点处自由壁的牵引
- Inward movement of the free wall
- No torsion or rotational movement.
没有扭转或旋转运动。
# Function of the Right Ventricle 右室的功能
- Maintains adequate PA perfusion pressure to improve gas exchange
维持足够的肺动脉压,以改善气体交换 - Maintains a low systemic venous pressure to prevent congestion of tissue or organs
维持较低的中心静脉压,以防止组织或器官充血 - Impaired RV results in reduced LV preload
右室功能受损导致左心室前负荷减少 - Ventricular interdependence.
心室相互依赖
# Ventricular Interdependence 心室相互依赖
- Around 40% of RV Systolic function is attributable to LV systolic function due to ventricular interaction
由于心室相互作用,约 40% 的右室收缩功能归因于左室收缩功能 - Ventricular interdependence can be direct or indirect
心室相互依赖可以是直接的,也可以是间接的- Direct: Via the septum and pericardium
直接的包括:通过间隔和心包作用 - Indirect: Via closed loop circulation i.e. RV output is equal to LV output.
间接的包括:通过闭环循环,即 RV 输出等于 LV 输出。
- Direct: Via the septum and pericardium
- Volume overload 容量过度负荷
- Flattening of septum in diastole
舒张期间隔变平 - Pressure overload 压力过度负荷
- Flattening of septum in systole and diastole
收缩期和舒张期间隔变平
# Difficulties in Assessment 右室评估的困难点
- Difficult to estimate RV volume due to crescent shape i.e. asymmetrical
由于新月形,即不对称,难以估计 RV 容积 - Difficult to estimate border due to trabeculation
由于肌小梁的存在,很难估计心内膜的边界 - Difficult to image as posterior to sternum
胸骨后方难以成像 - Difficult to image infundibulum which contains 25-30% of the RV volume.
漏斗部占右室体积的 25%-30%,这部分难以成像。
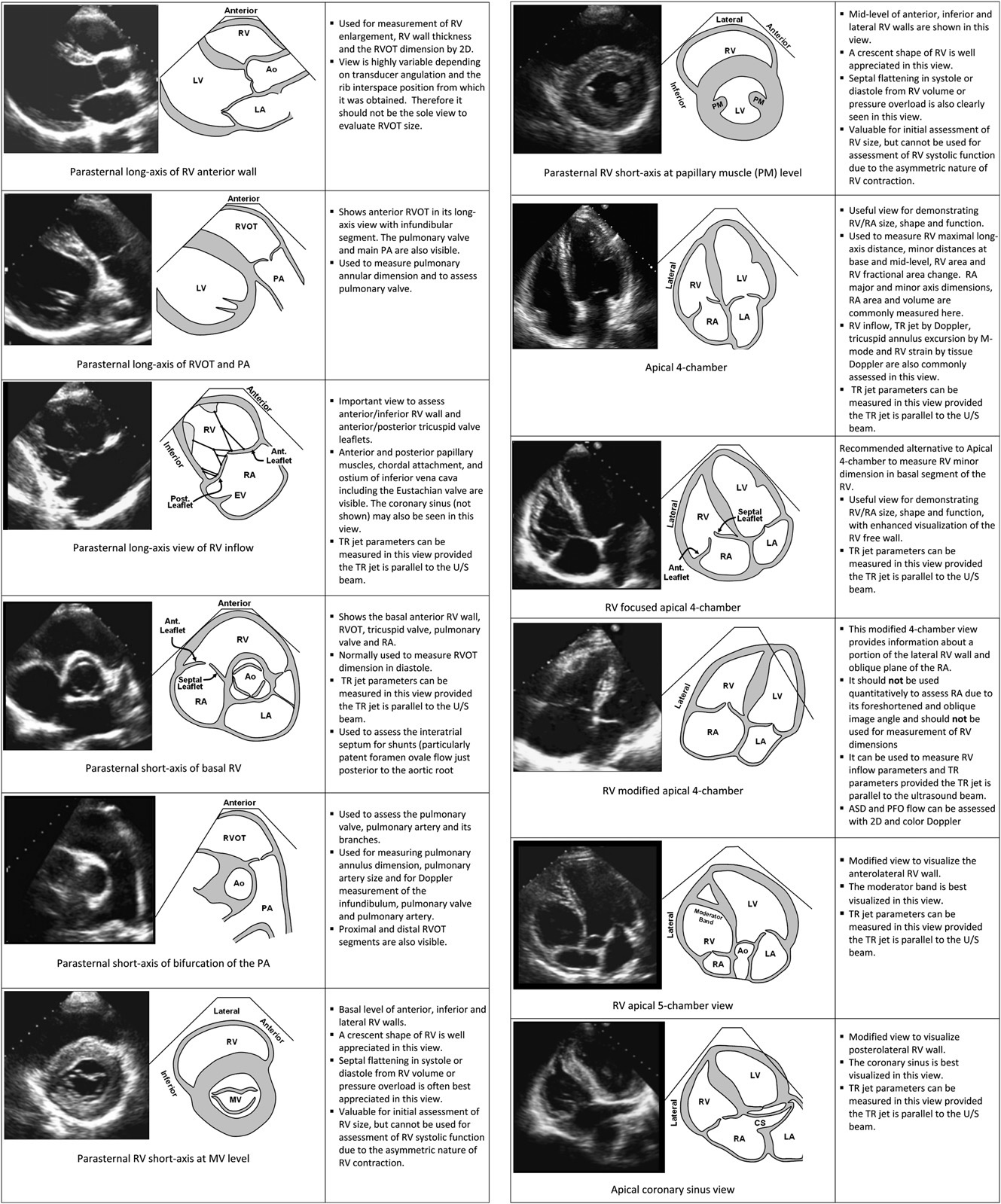
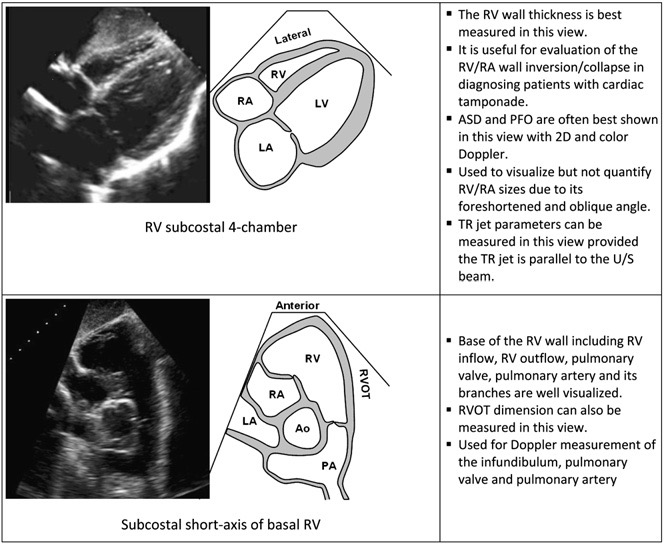
# Basics Views of the Right Ventricle [1]
# Dimensions and thickness of the RV
# RV inflow Dimensions

- Diagram (left) and corresponding echocardiographic apical 4-chamber image (right) showing the right ventricular (RV) basal (RVD1) and mid cavity (RVD2) RV minor dimensions and the RV longitudinal dimension (RVD3).
图 (左) 和相应的心尖四腔图 (右) 显示右室 (RV) 基底部 (RVD1) 和中部 (RVD2) 的 RV 最小尺寸和 RV 的纵向的长径 (RVD3)。 - The transducer is adjusted to focus on the RV chamber, with the goal of maximizing RV chamber size.
传感器被调整为聚焦在 RV 腔,以最大化 RV 腔的大小。 - The RV free wall is better seen in this view, also facilitating measurements for fractional area change.
在这张图中可以更好地看到 RV 游离壁,也便于测量面积变化分数。
| RV inflow Dimensions | 正常参考范围 | |
|---|---|---|
| Base (RVD1) 右心室内径,基底部 | Below the TV annulus | < 4.2cm |
| Mid (RVD2) 中部的 | Mid-RV | < 3.5cm |
| Length (RVD3) 右心室长径 | Base to apex | < 8.6cm |
# RV outflow Dimensions
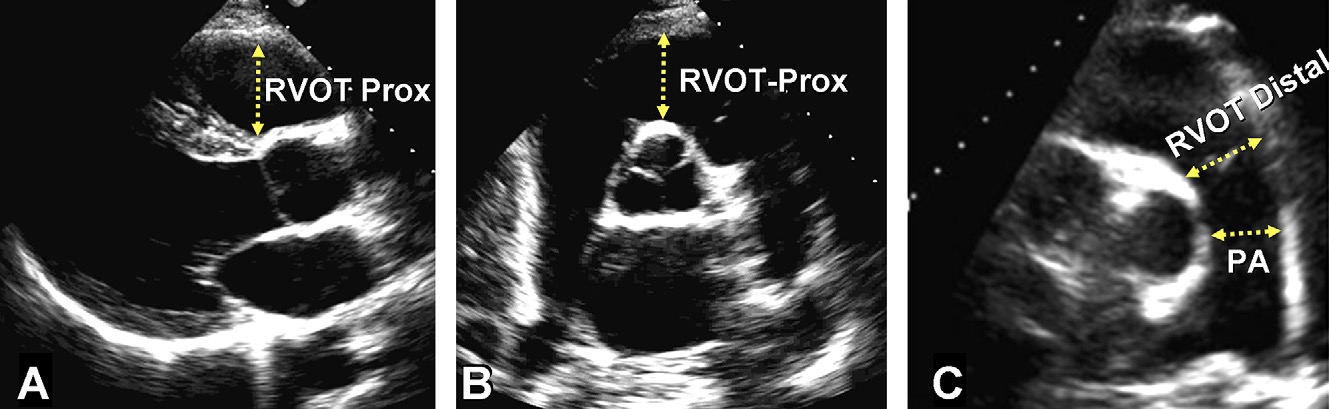
- Measurement of right ventricular outflow tract (RVOT) dimensions at the proximal or subvalvular level (RVOT-Prox) and at the distal or pulmonic valve (RVOT-Distal) in the (A) parasternal long-axis RVOT anterior portion view, (B) basal parasternal short-axis view, and (C) parasternal short-axis of pulmonary bifurcation view.
在 (A) 胸骨旁长轴 RVOT 前部切面、(B) 胸骨旁基底部短轴切面、(C) 胸骨旁肺分叉切面,测量右室流出道 (RVOT) 近端 / 瓣下水平 (RVOT-Prox) 和远端 / 肺动脉瓣水平 (RVOT-Distal) 的内径。 - PA, Pulmonary artery dimension between valve and the bifurcation point.
PA,瓣膜和分叉点之间的肺动脉内径。
| RV outflow Dimensions | 正常参考范围 | |
|---|---|---|
| Parasternal long axis | RVOT proximal in PLAX 右室流出道近端内径 | < 3.1cm |
| Parasternal short axis | RVOT proximal at AV level 右室流出道近端内径 | < 3.6cm |
| RVOT distal at PV level 右室流出道远端内径 | < 2.8cm | |
| PA diameter 肺动脉内径 | < 2.3cm | |
探头的位置对 RVOT 的测量影响很大,因此应该进行多个切面的测量,而不依靠单一的指标
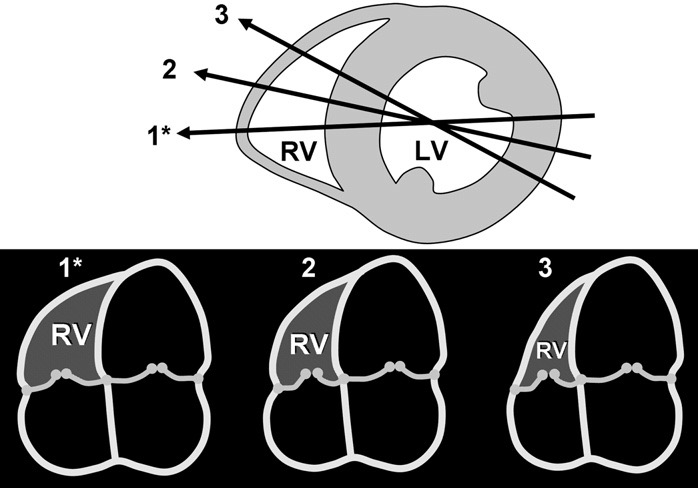
Diagram showing the recommended apical 4-chamber (A4C) view with focus on the right ventricle (RV) (1*) and the sensitivity of right ventricular sizewith angular change (2,3) despite similar size and appearance of the left ventricle (LV).
图中显示了推荐的心尖四腔(A4C)视图,聚焦右心室(RV)(1*)和随着角度变化,右心室大小变化明显(2、3),尽管左心室(LV)的大小和外观相似。
The lines of intersection of the A4C planes (1*,2,3) with a mid left ventricular short-axis are shown above and corresponding A4Cviewsbelow.
A4C 平面(1*、2、3)与左心室中段短轴的交点如上图所示,相应的 A4C 视图如下图所示。
# RV wall thickness 右心室室壁厚度
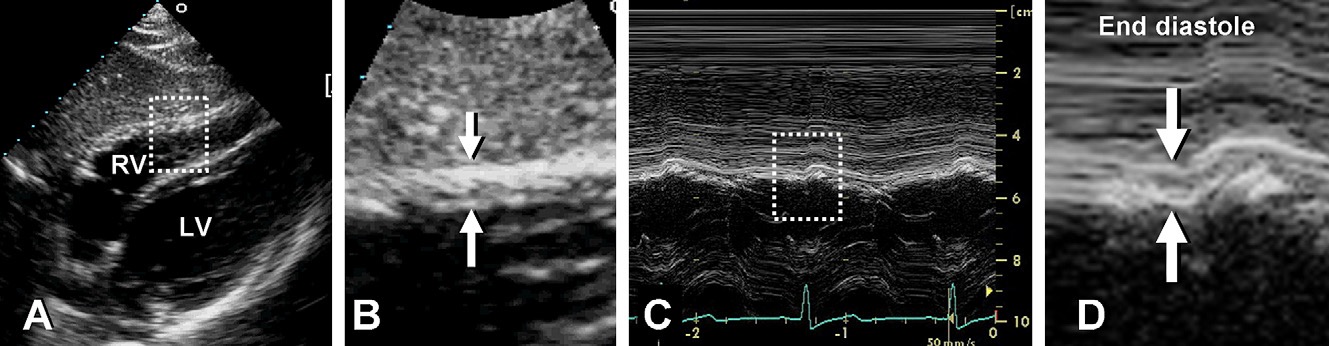
Measurement of end-diastolic right ventricular wall thickness.
舒张末期右心室壁厚度的测量。(A) Subcostal 2-dimensional image of right ventricular wall.
右室壁的剑突下二维图像。取样线与室壁呈垂直状态。(B) Zoom of region outlined in (A) with right ventricular wall thickness indicated by arrows.
放大 (A) 中线框的区域,右室壁厚度用箭头表示。(C) M-mode image corresponding to arrows in (B).
与 (B) 中的箭头相对应的 M 模式图像。(D) Zoom of region outlined in (C) with arrows indicating wall thickness at end-diastole.
放大 (C) 中概述的区域,箭头指示舒张末期的壁厚。Assessed in parasternal subcostal or parasternal long axis
剑突下或胸骨旁长轴的评估Measure at level of TV chordae at R wave
在 R 波的 TV 腱索水平测量RV hypertrophy due to chronic pulmonary hypertension(PH), hypertrophic cardiomyopathy(HCM), infiltrative cardiomyopathy
右室肥厚的常见病因:慢性肺动脉高压、肥厚性心肌病、限制型心肌病,心肌淀粉样变
| RV thickness | 参考范围 |
|---|---|
| Normal | < 5mm |
# Assessing RV function
# Fractional Area Change 面积变化分数
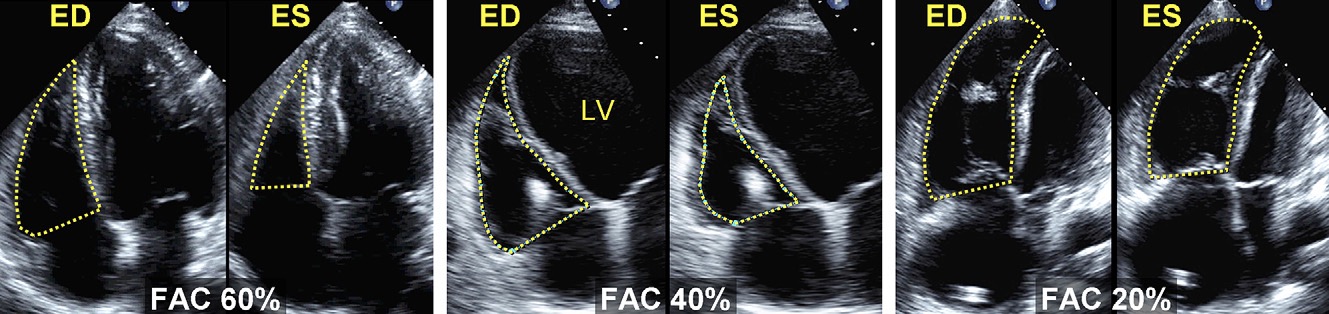
Examples of right ventricular fractional area change (FAC).
The endocardial border is traced in apical 4-chamber (A4C) views from the tricuspid annulus along the free wall to the apex, then back to the annulus, along the interventricular septum at end-diastole (ED) and end-systole (ES).
在舒张末期(ED)和收缩末期(ES),心内膜边界在心尖四腔(A4C)切面中,从三尖瓣环沿着游离壁到心尖,然后沿着室间隔返回瓣环。Trabeculation, tricuspid leaflets, and chords are included in the chamber.
心腔内有肌小梁、三尖瓣瓣叶和和腱索。(Left) Normal subject, FAC 60%. (Middle) Moderately dilated right ventricle (RV), FAC 40%, and a markedly dilated left ventricle (LV).
(左) 正常受试者,FAC 60%。(中) 右心室 (RV) 中度扩张,FAC 为 40%,左心室 (LV) 明显扩张。(Right) Dilated RV, FAC 20%, and the LV is foreshortened as a result of optimizing the view for the right ventricular chamber.
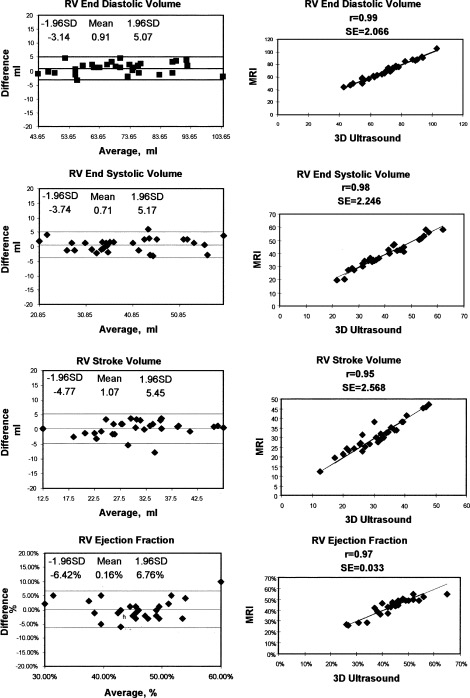
(右) 右室扩张,FAC 为 20%,由于优化了右室切面,LV 看起来缩短了。Well correlated with RV function measured in MRI
与 MRI 测量的右室功能相关性良好Must have good RV tracing to measure FAC accurately
RV 必须描绘良好才能准确测量 FAC
| FAC | 参考范围 |
|---|---|
| Normal | 32 - 60% |
| Mild impairment | 25 - 31% |
| Moderate impairment | 18 - 24% |
| Severe impairment | ≤17% |
# RV Ejection Fraction 右室射血分数
# Method one: Area-length
- Under-estimates EF - therefore, not routine
会低估 EF - 因此,不是常规操作 - Assumes RV is symmetrical;
此公式假设 RV 是对称的(但实际并不是对称的); 。
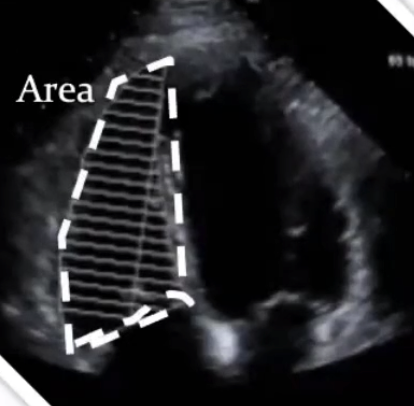
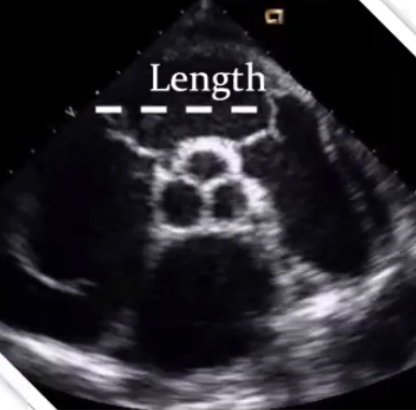
- 胸骨旁短轴进行长度的测量
- 用改良的心尖四腔进行面积的测量
- 根据这个方法可以达到右室的舒张末容积和收缩末容积
# Method two: Simpsons EF
- Assumes the RV is symmetrical
假设 RV 是对称的(但实际是不对称的) - Does not include the infundibulum (which may be
25% of the RV volume)
不包括漏斗部分的测量(可能占 RV 容积的 25%) - Avoid this technique for assessment of the RV.
避免使用这种技术来评估右室,仅供了解,临床不常用
It works well for the LV as the structure is symmetrical with orthogonal view in apical 4 and apical 2chamber.
此方法适用于 LV,因为左室的结构在心尖四腔和心尖两腔中是相对对称的正交视图,但右室不一样,右室是新月形的不对称的。
# The problem
- The RV is not symmetrical 右室是不对称的
- Therefore, real time 3D echocardiography (RT3DE) is needed to estimate volumes accurately.
因此,如果觉得 RVEF 有下降,除了二维超声,还应运用实时三维超声心动图 (RT3DE) 来准确估计右室容量,或 MRI 来对右室功能进行进一步评估 - Are both functional and prognostic parameters
右室功能对患者预后非常重要,既是功能参数又是预后参数
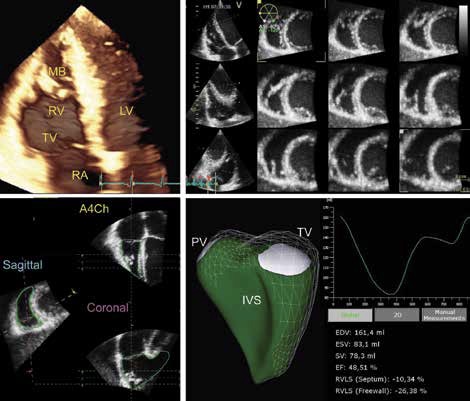
| 正常参考范围 | |
|---|---|
| RVEDV (ml) 右室舒张末期容积 | 86±21 |
| RVEDVI (ml/m2) | 49±10 |
| RVESV (ml) 右室收缩末期容积 | 29±11 |
| RVESVI (ml/m2) | 16±6 |
| RVEF (%) | 67±8 |
# TAPSE (Tricuspid Annular Plane Systolic Excursion) 三尖瓣环平面收缩期偏移

, referred to as TAPSE, is indicated by the arrow.")
- Apical 4 chamber window
心尖四腔切面 - Degree systolic excursion of the tricuspid annulus
三尖瓣环的收缩期偏移 - Reproducible.
有较好的可重复性 - 临床上更多应用的是 TAPSE 和面积变化分数来评估右室功能
| TAPSE | 参考范围 |
|---|---|
| Normal | ≥ 16mm |
| Mild impairment | 13 - 15mm |
| Moderate impairment | 10-12mm |
| Severe impairment | < 10mm |
# Tei Index 心肌做功指数
- Tei index = RV myocardial performance index (MPI)
心肌做功指数 = 心肌综合指数(MPI),科研中常用 - Pulse wave doppler at tricuspid valve inflow
使用脉冲多普勒采样三尖瓣流入端,获得 PWD-MPI - Marker of both global systolic and diastolic function.
反映整体收缩和舒张功能
| Isovolumic contraction time | IVCT | 等容收缩时间 |
| Isovolumic relaxation time | IVRT | 等容舒张时间 |
| Ejection time | ET | 射血时间 |
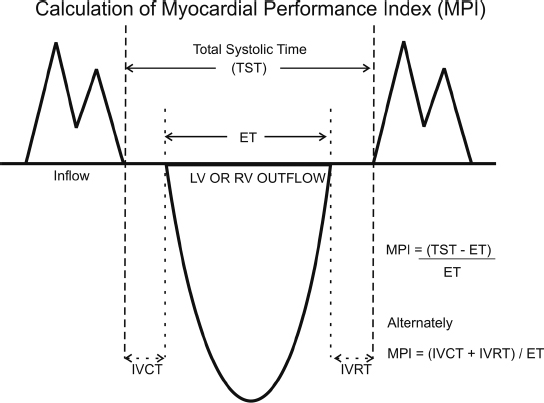
- Schematic outlining calculation of the myocardial performance index (MPI).
心肌性能指数(MPI)计算示意图。 - The myocardial performance index is the ratio of the sum of the isovolumic contraction and relaxation times (IVCT, IVRT) to ejection time (ET).
心肌性能指数是等容收缩和舒张的时间(IVCT、IVRT)之和与射血时间(ET)之比。 - It can be calculated by subtracting ET from total systolic time (TST) as noted in the two alternate formulas.
如两个替代公式所述,可以通过从总收缩时间(TST)中减去 ET 来计算。
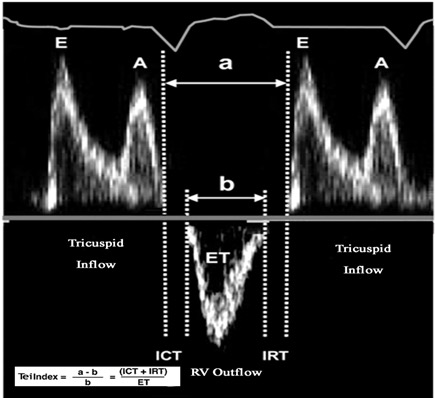
- (a) 从三尖瓣关闭(A 波),至下一个心动周期三尖瓣打开(E 波)的时间 [4]
- (b) 射血时间
| Tei index/MPI | 参考范围 |
|---|---|
| PWD-MPI | ≤ 0.4 |
# Tissue Doppler Imaging (TDI): S' 组织多普勒成像
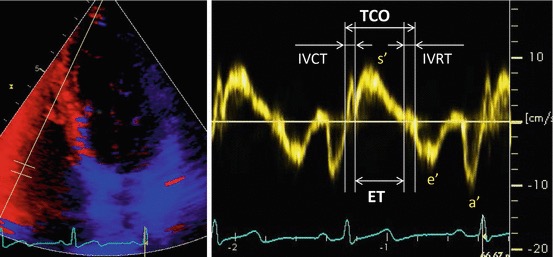
- Assess in apical 4 chamber window
在心尖四腔切面评估 - Pulsed wave doppler (with TDI) in the middle of the basal segment of the RV free wall
脉冲波多普勒 (带组织多普勒),取样容积放在右室游离壁、基底段中间,靠近三尖瓣瓣环的地方,获得 TDI-MPI - s' is the highest systolic velocity
s' 是收缩期位移的最高速度
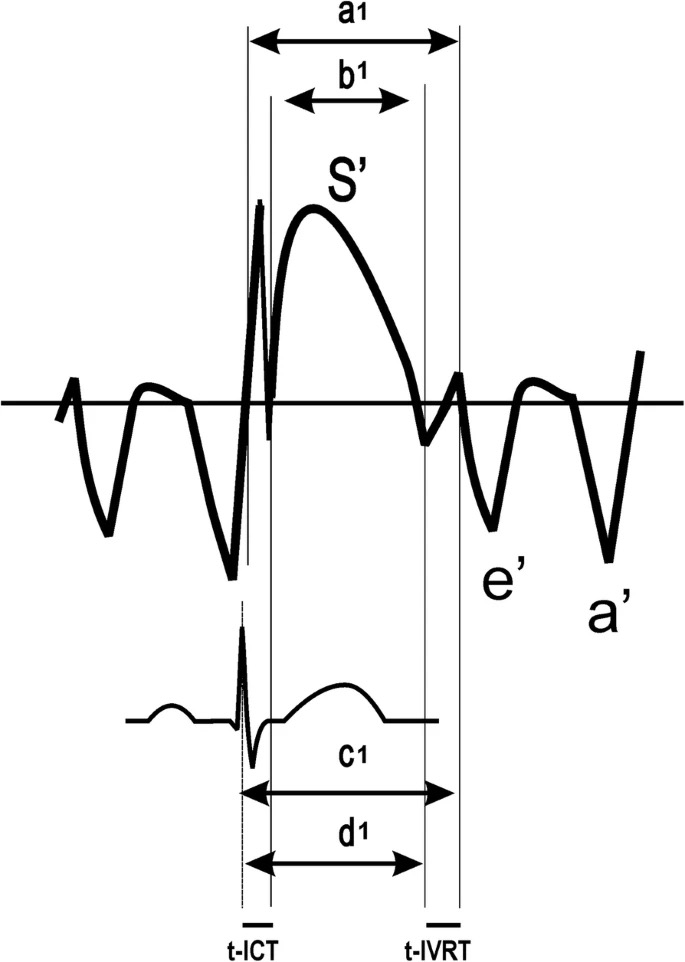
- Scheme for measurement of time intervals used to calculate the tissue Doppler-derived myocardial performance index (TDI-MPI): [5]
用于计算组织多普勒导出的心肌性能指数的时间间隔的测量方案- a, time from cessation of the a’ wave to the onset of the e’ wave;
从 a' 波停止到 e' 波开始的时间; - b, the duration of the S wave;
S 波的持续时间; - c, interval between the R wave and onset of the e’ wave;
R 波与 e' 波起始点之间的距离; - d, interval between the R wave and cessation of the S wave;
R 波与 S 波终点之间的距离; - ICT, tissue Doppler-derived isovolumetric contraction time; IVRT, isovolumetric relaxation time
ICT,组织多普勒获得的等容收缩时间;IVRT 等容舒张时间
- a, time from cessation of the a’ wave to the onset of the e’ wave;
| TDI | 提示右室功能正常 |
|---|---|
| s' | ≥ 12cm/s |
| TDI-MPI | < 0.55 |
- Evidence based importance in conditions affecting RV function e.g. inferior MI affecting the RV
影响 RV 功能的条件下基于证据的重要性,例如下壁心肌梗死对 RV 的影响 - Limitations: 限制
- Tricuspid valve disease (tricuspid stenosis, tricuspid regurgitation, TS / TR/ annuloplasty)
当存在三尖瓣疾病时(三尖瓣狭窄 / 三尖瓣反流 / 瓣环成形术)对 s' 影响较大 - Only evaluates basal segment of RV
仅评估了右心室基底段,不能反应整体情况 - Affected by doppler alignment
对多普勒采样线有角度依赖,测量值不一定准确
- Tricuspid valve disease (tricuspid stenosis, tricuspid regurgitation, TS / TR/ annuloplasty)
# Assessing RV systolic pressure
# Pulmonary Artery Systolic Pressure 肺动脉收缩压
- 肺动脉收缩压 = 右心室收缩压 = 最大三尖瓣跨瓣压差 + 右房压
- In the absence of RVOT obstruction
在没有右室流出道梗阻的情况下
- In the absence of RVOT obstruction
| 肺动脉收缩压 | 参考范围 |
|---|---|
| Normal | 18 to 25 mmHg |
| Mild | 30 to 40 mmHg |
| Moderate | 40 to 70 mmHg |
| Severe | > 70 mmHg |
# TR Doppler jet 三尖瓣反流多普勒曲线
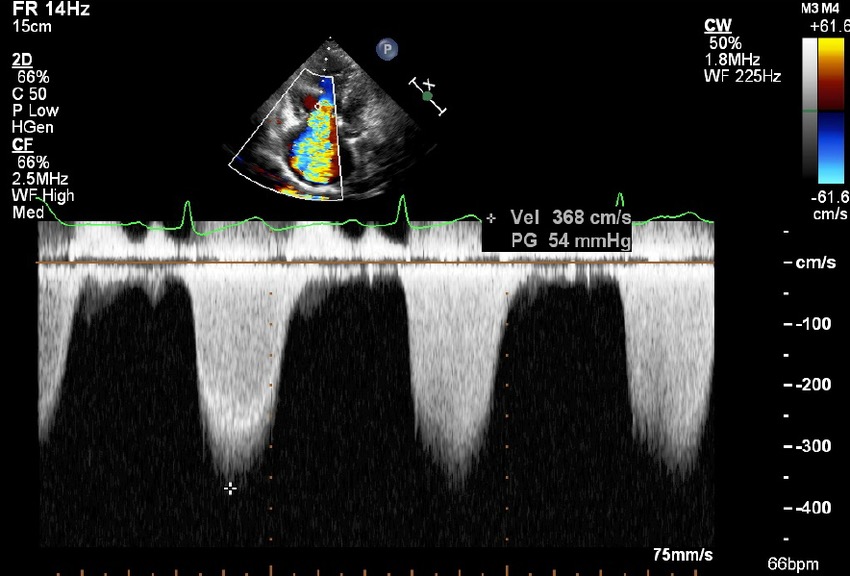
2D Echocardiogram apical view with color Doppler showing severe tricuspid regurgitation, with continuous wave Doppler showing pressure gradient of 54 mm Hg across tricuspid valve [6]
Best assessed in parasternal RV inflow, parasternal short axis or apical four chamber.
最好在胸骨旁右室流入道、胸骨旁短轴或心尖四腔进行评估。从多个切面获得最大的三尖瓣频谱图进行描绘。
使用连续多普勒,可以在二维及彩色多普勒的指引下放置取样线,获得最清晰的、密度最高的三尖瓣反流频谱度。
取最大值作为 TR 的最大反流速度。
# Bernoulli Equation 伯努利方程
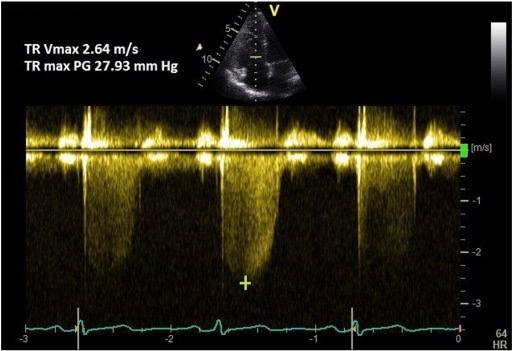
When fluid passes through a narrow space, the velocity increases.
当流体通过一个狭窄的空间时,速度会增加。Pressure is increased before the obstruction and is low behind the obstruction.
压力在阻塞之前增加,而在阻塞之后降低。The difference between these pressures is known as the pressure gradient which can be calculate using the Bernoulli equation.
这些压力之间的差值称为压差 / 压力梯度,可以使用伯努利方程计算。简化的伯努利方程式:
In the example above: [7]
which is the pressure change between the RV and RA
这是 RV 和 RA 之间的压力变化,也就是跨三尖瓣的压差
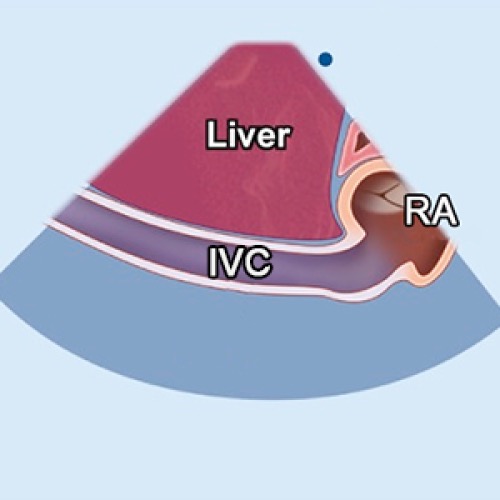
# Estimate Right Atrial Pressure (RAP) 右房压
- Obtain the IVC in subcostal window
在剑突下声窗获得下腔静脉 - Ask the patient to sniff - mimics inspiration - and assess collapsibility of the IVC
让病人深呼吸,并评估下腔静脉的崩溃 / 塌陷


| 1️⃣ Size of IVC | 2️⃣ IVC size On Inspiration | Right atrial pressure(mmHg) |
|---|---|---|
| Small < 1.5cm | Near total collapse | 0 - 5 |
| Normal(1.5-2.5cm) | Decrease > 50% | 5 - 10 |
| Normal | Decrease < 50% | 10 - 15 |
| Dilated > 2.5cm | Decrease ≤ 50% | 15 - 20 |
| Both IVC & Hepatic veins dilated | No change | > 20 |
# RV strain 右室应变
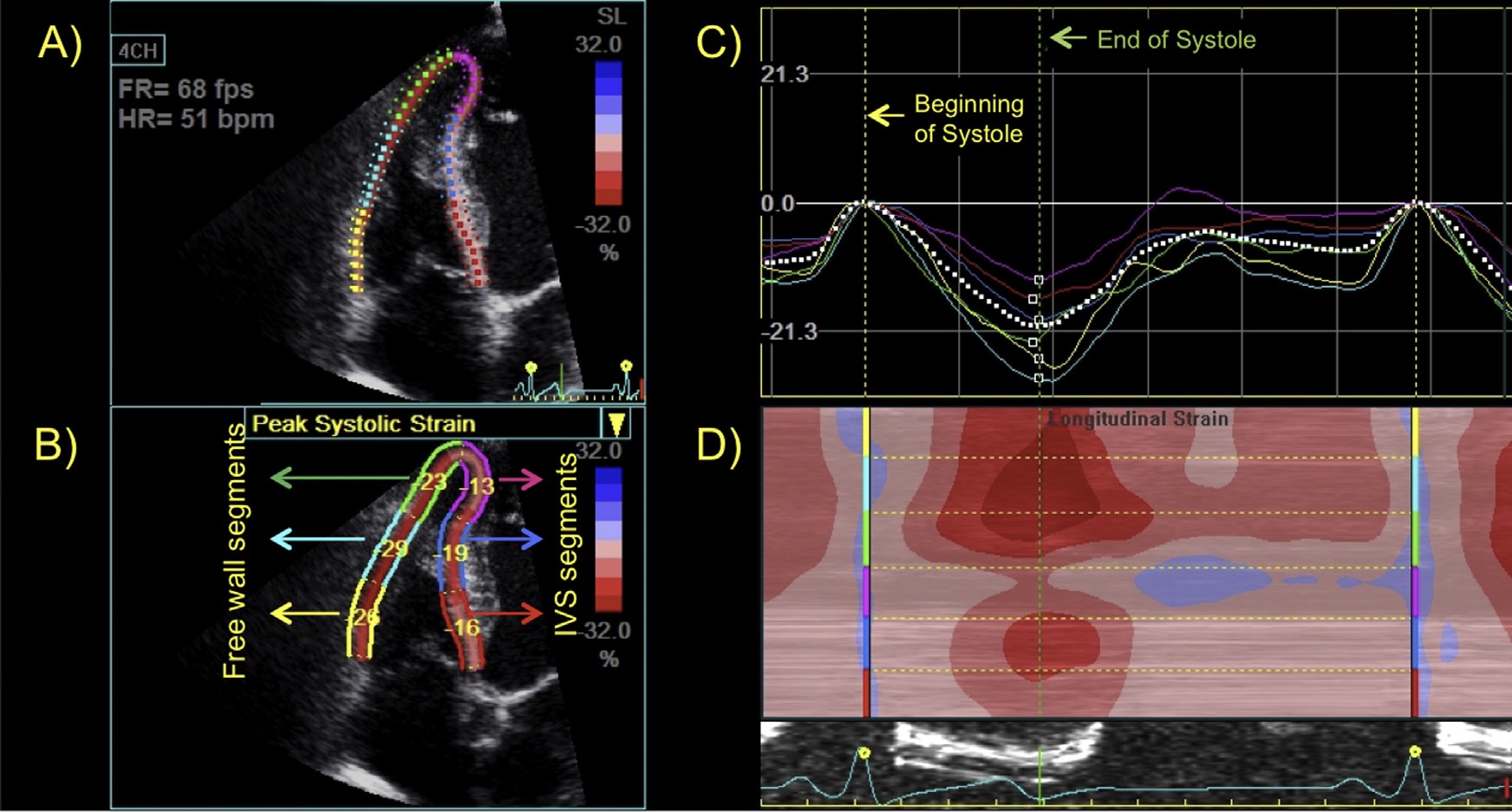
Speckle-tracking echocardiography to evaluate RV function. 斑点追踪超声心动图评估 RV 功能。 RV strain in Apical 4 Chamber [8]
Angle independent assessment using 2D pictures
利用二维图像进行角度独立评估Measures global and segmental function
衡量全局和节段功能The degree of change in myocardial deformation
心肌变形的变化程度Strain rate = rate of deformation over time
应变率 = 随着时间推移的变形率Not routine part of RV assessment currently.
目前不是 RV 评估的常规部分。
| 正常参考值 | |
|---|---|
| RV global strain | -24.5 ± 3.8 |
| RV free wall strain | -28.5 ± 4.8 |
# Caution with 2D Parameters 注意事项
TAPSE
- Load and angle dependant
有负荷和角度的依赖性 - Assumes that the TV annulus represents the entire RV
假设三尖瓣瓣环代表整个右室
- Load and angle dependant
FAC
- Load dependant
负荷依赖 - Heavily trabeculated RV - border challenging to trace
排除右室过多的肌小梁导致的边界难以描绘
- Load dependant
Tei Index
- Load dependant
负荷依赖 - Unreliable in AF
在房颤中不可靠 - False negatives if high right atrial pressure
如果右房压高,则出现假阴性
- Load dependant
Longitudinal Strain
纵向应变- Load dependant
负荷依赖性
- Load dependant
Rudski, L. G. et al. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography. Journal of the American Society of Echocardiography 23, 685–713 (2010). ↩︎
Surkova, E., Peluso, D., Kasprzak, J. D. & Badano, L. P. Use of novel echocardiographic techniques to assess right ventricular geometry and function. Kardiologia Polska (Polish Heart Journal) 74, 507–522 (2016). ↩︎
Niemann, P. S. et al. Anatomically Oriented Right Ventricular Volume Measurements With Dynamic Three-Dimensional Echocardiography Validated by 3-Tesla Magnetic Resonance Imaging. Journal of the American College of Cardiology 50, 1668–1676 (2007). ↩︎
D, S. & Vanajakshamma, V. The Immediate and Short Term Impact of Successful Percutaneous Transvenous Mitral Commissurotomy on Right Ventricular Function. Journal of Cardiovascular Diseases & Diagnosis 03, (2015). ↩︎
Fernandes, J. M. G. et al. Clinical value of myocardial performance index in patients with isolated diastolic dysfunction. Cardiovasc Ultrasound 17, 1–9 (2019). ↩︎
Khandelwal, G., Ruhela, M. & Bagarhatta, R. Mystery of the Right Sided Heart Failure in a Young Patient. American Journal of Medical Case Reports 2, 94–96 (2014). ↩︎
Parasuraman, S. et al. Assessment of pulmonary artery pressure by echocardiography—A comprehensive review. IJC Heart & Vasculature (2016). ↩︎
Moreira, H. T. et al. Right Ventricular Systolic Dysfunction in Chagas Disease Defined by Speckle-Tracking Echocardiography: A Comparative Study with Cardiac Magnetic Resonance Imaging. J Am Soc Echocardiogr 30, 493–502 (2017). ↩︎