# Clinical Cases Part 1
# Case 1
![]()
![]()
Mild, moderate or severe LV systolic dysfunction?
Severe
What is wrong with the interventricular septum?
scarred
What can be seen with LV contrast?
Thrombus or Clot
# Case 2
![]()
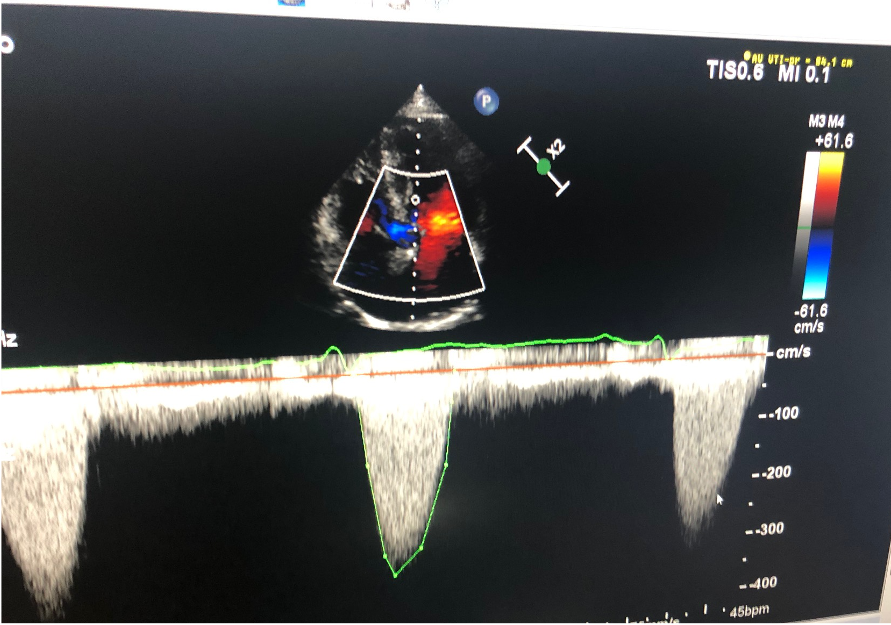
- What do we think is the cause of the doppler trace?
Aortic Stenosis
![]()
![]()
Is the aortic valve normal or abnormal?
Abnormal
Is the aorta normal or abnormal?
Normal
Is the colour doppler normal or abnormal?
Abnormal
# Case 3
![]()
Is LV function normal or abnormal?
Normal
![]()
Are there LV wall motion abnormalities?
Yes (Apical inferior/Anterior)
![]()
Are there LV wall motion abnormalities?
Yes (anterior/septal)
![]()
Are the wall motion abnormalities?
Yes (middle Apical inferior/anterior)
Is there LV thrombus?
No
# Case 5
![]()
What is the highlighted feature?
LV Gradient
What is the diagnosis?
Apical Hypertrophic Cardiomyopathy
![]()
What are the abnormalities?
LV Hypertrophy, Systolic Anterior motion (SAM) of Mitral Valve
What is the diagnosis?
Hypertrophic Cardiomyopathy
# Quiz
The next operation?
![]()
- Needs urgent pericardiocentesis
- Await surgery
- Diuretics are used with a pericardial effusion
- Shows possible heart failure.
Which is true
![]()
- Normal aortic and mitral valve
- TAVI valve, well seated
- Low TAVI valve
- Shows normal mitral valve.
Which is true
- Mitraclip is used in pts with I.E.
- Mitraclip used in rheumatic heart disease
- Mitraclip is optimal in pts with functional mitral regurgitation
- Mitraclip is first choice in low risk patients as it is non-invasive.
Which is true
![]()
- This shows AR of the aortic valve
- This shows central regurgitation
- This shows paravalvular AR
- Pt should have a paravalvular plug inserted
Which is true
![]()
- This shows primary MR
- This shows central regurgitation
- This is suitable for mitraclip
- LV function is likely to be normal.
Which is true
![]()
- This shows tamponade
- Shows RV diastolic collapse
- This is suitable for mitraclip
- LV function is normal.
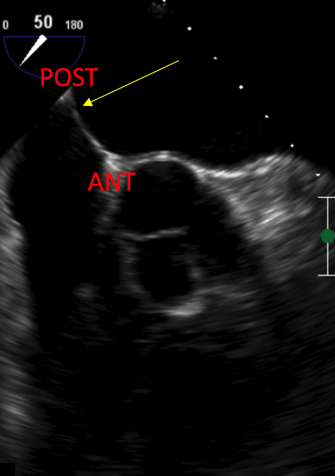
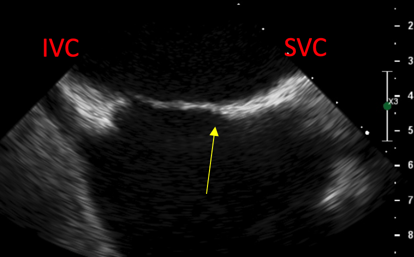
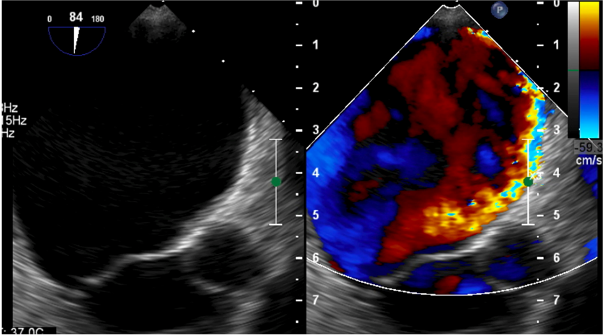
Where is the septum punctured?
![]()
![]()
- Anterior and superior
- Posterior and superior
- Anterior and inferior
- Posterior and inferior
Which is true
![]()
- The speed of accumulation is the most important
- If the size is > 1.5cm effusion should be drained urgently
- There is a fall in BP on expiration > 30mmHg
- If there is tamponade without inflammatory signs, it is more likely to be due to cancer.
Which is true
![]()
![]()
- This shows functional mitral regurgitation
- This shows eccentric mitral regurgitation
- This shows central regurgitation
- This pathology is not amenable to clip.
Which is true
- If there is residual MR after clip insertion - Must operate
- If there is residual MR after clip, release and regrasp
- If there is residual MR after clip, insert a second clip
- Mitraclip is first choice in tissue MVR transvalvular regurgitation.
Which is true
![]()
- This shows a DCM
- This shows an athletes heart
- A dilated RV is due to an ASD
- The aorta is mildly dilated – This is normal.
Which is true
- TAVI is superior to surgery as overall less pacemaker insertion
- TAVI is superior to surgery as less vascular problems
- TAVI should be considered in moderate risk patients
- TAVI complications include perforation of the right ventricle
Which is true
![]()
- The LVOT VTI will be around 1m/s
- If the AV Vmax is 3m/s, pt should not be offered a TAVI
- This is an athletic heart
- There will likely be primary MR.
Which is true
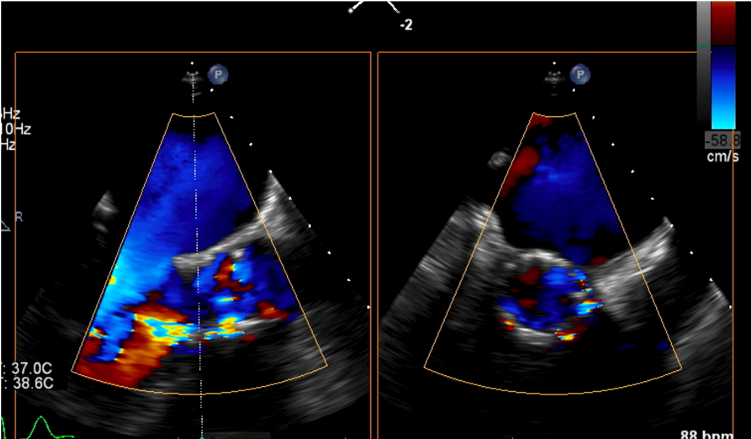
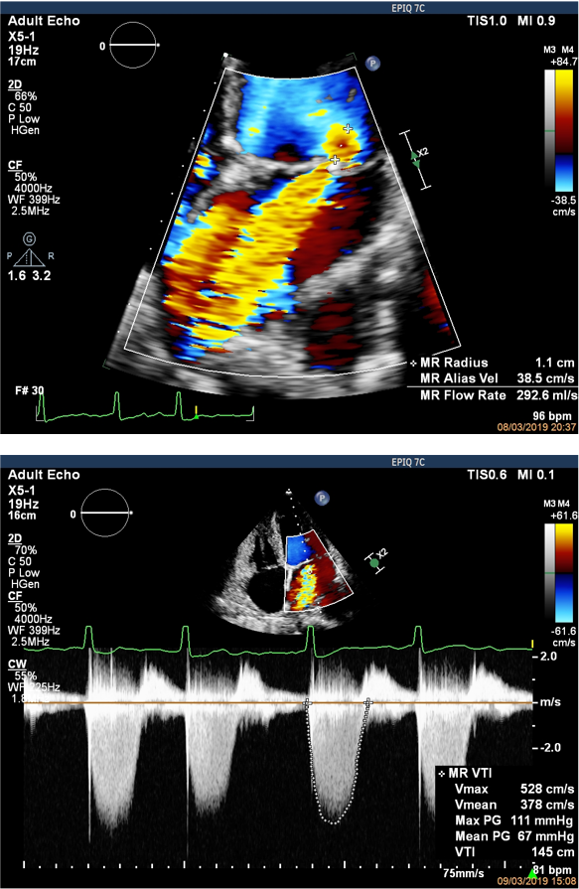
![]()
![]()
- There is no mitral regurgitation
- There is mild MR
- There is moderate MR
- There is severe MR
# Clinical Cases Part 2
# Case 1
A 62-year-old male presents to the medical unit with breathlessness.
ECG: LBBB
CXR: pulmonary oedema
You perform an echocardiogram.
![]()
The LVIDd measures at 6cm. What does the patient have?
- Normal LV
- Mildly dilated LV
- Moderately dilated LV
- Severely dilated LV
The LVIDs is 5.5cm. What is the fractional shortening?
![]()
What is the visual ejection fraction?
- 45-50%
- 35-40%
- 15-20%
- 20-25%
- 40-45%
The MAPSE is around:
![]()
- This patient has evidence of:
- Mild eccentric MR
- Severe functional MR
- Mild functional MR
- Moderate functional MR
![]()
A similar patient presents a few days later. What is the diagnosis?
- Moderate MR
- Severe MR
- Mild MR
- Moderate – severe MR
You review the patient’s diastolic function. The E/A ratio is 1.5, DT 200ms. E/E’ 16. The patient’s left atrium is 21cm2. The patient has evidence of:
- Normal diastolic function
- Mild diastolic dysfunction
- Moderate diastolic dysfunction
- Severe diastolic dysfunction
# Case 2
A 72-year-old female initially presented with chest pain. She is awaiting an angiogram.
ECG: Anterior ST elevation
CXR: Normal
You perform an echocardiogram.
![]()
This patient has RWMA consistent with:
- LAD infarction
- LCx infarction
- Takotsubo’s cardiomyopathy
- RCA infarction
What is the overall LV ejection fraction?
# Case 3
A 72-year-old male presents with a collapse episode.
ECG: Second degree AV block
CXR: Cardiomegaly, clear lung fields
You perform an echocardiogram.
![]()
- This patient has evidence of:
- Concentric LVH
- Cardiac sarcoidosis
- Cardiac amyloidosis
- Hypertrophic cardiomyopathy
- Severe systolic dysfunction
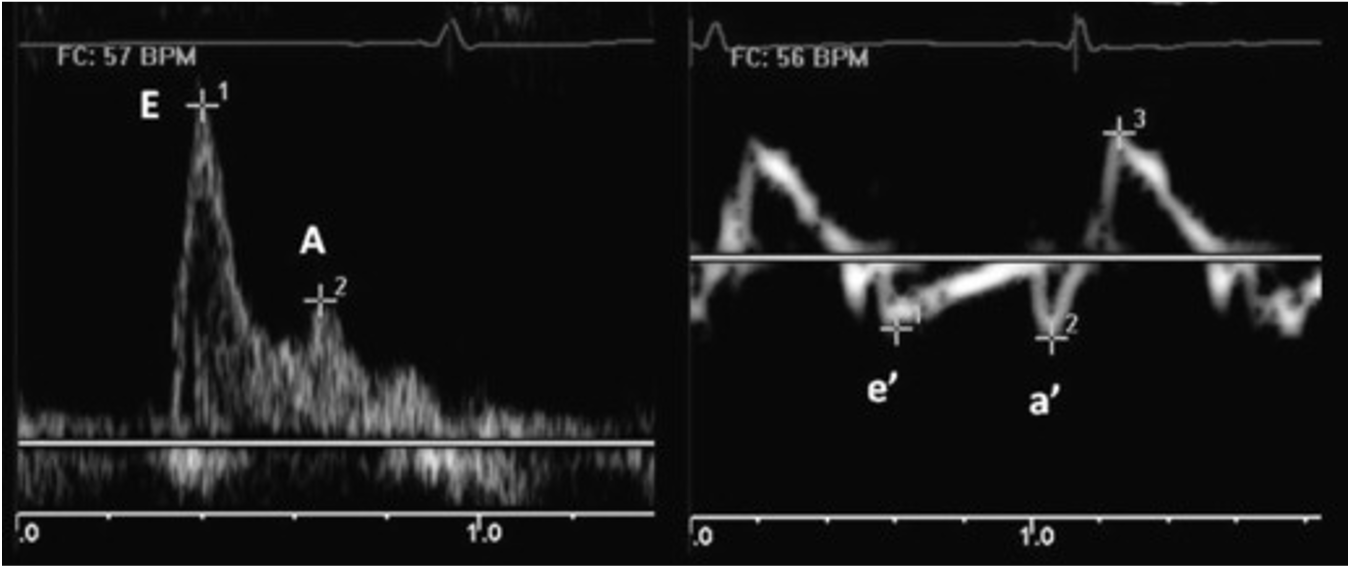
![]()
MV E peak 1.1 m/s
MV A peak 0.4 m/s
E’med 0.04 m/s
A’med 0.05 m/s
- Which of the following are true?
- E:A = 2.75
- E/E’ (med) = 27.5
- E/E’ (med) = 2.75
- This patient has restrictive diastolic function
- This patient has normal diastolic function
![]()
- What are the key features seen on this subcostal window?
- Normal wall thickness
- LV hypertrophy
- Thickened IAS
- Preserved systolic function
- RV hypertrophy
# Case 4
A 43-year-old male under investigation for breathlessness is referred for an echocardiogram. He had an abnormal CT of his chest.
ECG: AF
CXR: Hilar lymphaedenopathy
You perform an echocardiogram.
![]()
- This patient has evidence of:
- Severe left ventricle systolic dysfunction
- Thinned and akinetic inferoseptum
- Dilated left ventricle
- Dilated atria
![]()
- This patient has signs consistent with:
- Cardiac amyloidosis
- Normal echocardiogram
- Cardiac sarcoidosis
- Hypertrophic cardiomyopathy
- Haemosiderosis
# Case 5
An 82-year-old male presents with a stroke.
ECG: Normal sinus rhythm
CXR: Normal
You perform an echocardiogram.
![]()
What are the key findings on this image?
- Severe systolic dysfunction
- Global hypokinesia
- Apical thrombus
- Diastolic impairment
- Endomyocardial fibrosis