# Learning Obiectives
- Anatomy of the PV 解剖
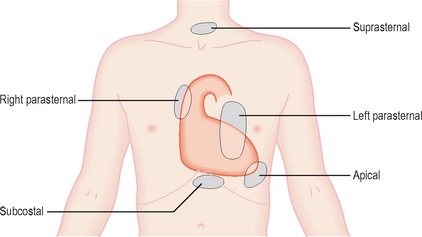
- Echocardiographic views to assess PV 超声切面
- Pathologies of the PV 病理学
- Assessment of severity of PV lesions 严重程度评估
# Pulmonary Valve (PV)
- Semilunar valve: separates RVOT from main PA
半月瓣:分隔右室流出道与肺动脉 - Anterior and superior to the aortic valve
位于主动脉瓣前上 - Trileaflet; but a "thinner' structure than the AV as it operates against a lower pressure
三叶瓣;肺动脉瓣的瓣膜厚度比主瓣要薄,因为它对抗的压力要比主瓣小;有时候超声短轴切面没法看清楚三个瓣 - Most disorders are congenital
大多数疾病是先天性的
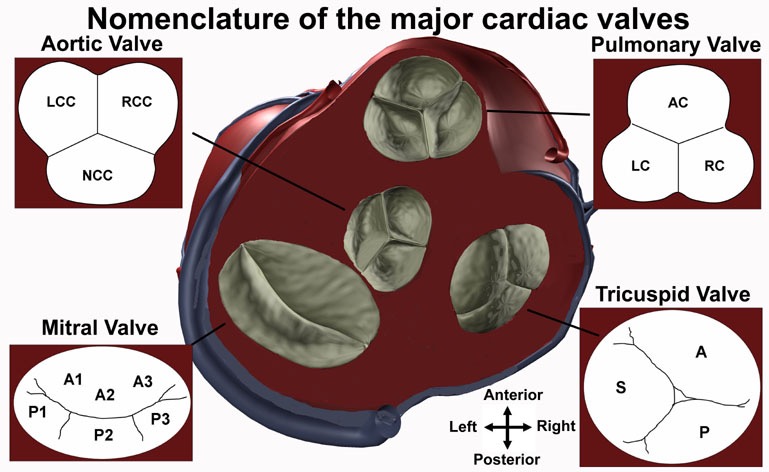
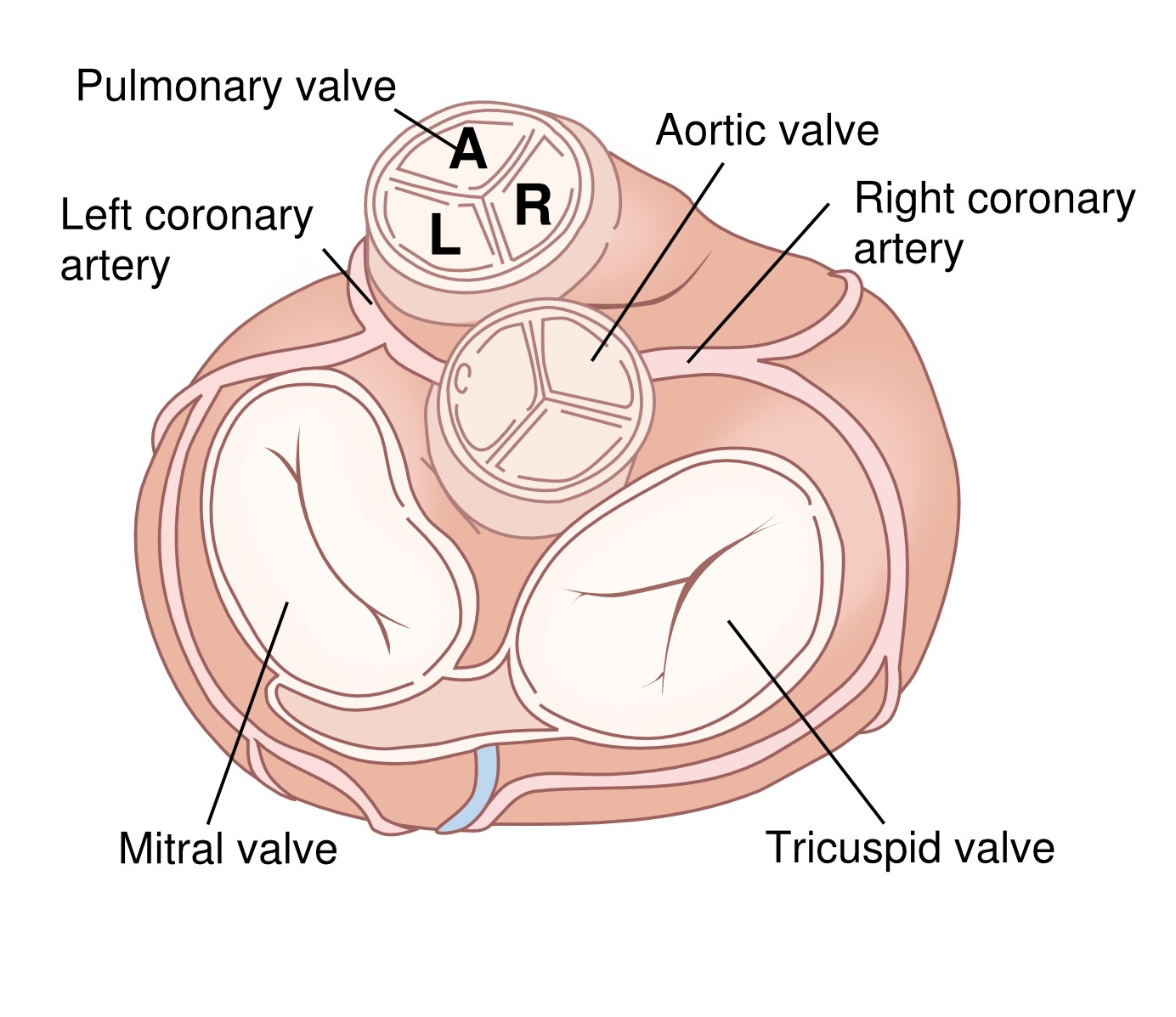
- The relative positions of the aortic, mitral, pulmonary, and tricuspid valves are shown in the diagram of the heart at the center of the figure.
主动脉瓣、二尖瓣、肺瓣和三尖瓣的相对位置如图中心的心脏图所示。 - The aortic valve has three cusps: the left coronary cusp (LCC), the right coronary cusp (RCC), and the non-coronary cusp (NCC).
- The mitral valve has an alphanumeric nomenclature that numbers from the anterior to the posterior, with respect to the heart, and attaches an A or a P in front of the anterior or posterior leaflets, respectively (A1-A3, P1-P3).
- The pulmonary valve has three cusps: the anterior cusp (AC), the left cusp (LC), and the right cusp (RC).
- The tricuspid valve has three leaflets named the anterior (A), septal (S), and posterior (P).
# Pulmonary Stenosis (PS)
- Prevalence 8/10,000 live births
发病率 - Site of stenosis 狭窄部位
- Valvular 瓣膜
- Sub valvular: (RVOT obstruction)
瓣下(右室流出道狭窄) - Supra valvular
瓣上
- Severity of stenosis 狭窄的严重程度
- Aetiology of stenosis 狭窄的病因(风湿性或其他)
- Ancillary findings: i.e RV hypertrophy
辅助发现:即右室肥厚
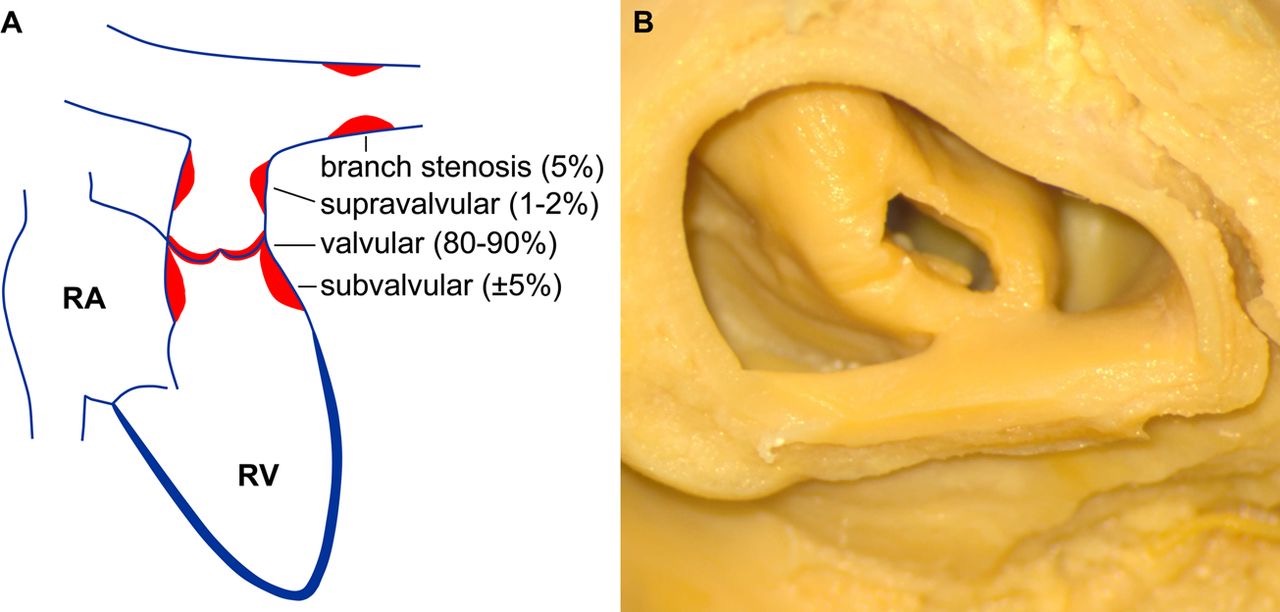
Table 1 Common genetic syndromes associated with pulmonary stenosis [1]
与肺动脉狭窄相关的常见遗传综合征
Syndrome | Genetic defect | Cardiac features | Non-cardiac features |
|---|---|---|---|
Noonan | PTPN11, SOS1, aberrant RAS-MAPK-signalling, heterogeneous trait | Dysplastic pulmonary valve stenosis, supravalvular pulmonary stenosis, hypertrophic cardiomyopathy | Short stature, hypertelorism, downward eye slant, low set ears |
Williams-Beuren | 7Q11.23 deletions, autosomal dominant trait | Supravalvular aortic or pulmonary stenosis | Elfin face, short stature, impaired cognition and development, endocrine disorders, genitourinary abnormalities |
Leopard | PTPN11, RAF-1, autosomal dominant trait | Electrocardiographic abnormalities, supravalvular or valvular pulmonary stenosis | Lentigines, ocular hypertelorism, abnormal genitalia, retardation of growth, deafness |
DiGeorge (velocardiofacial) | 22011 deletion, autosomal dominant trait | Conotruncal defects such as tetralogy of Fallot, interrupted aortic arch, truncus arteriosus, vascular rings and ASD/VSD | Hypertelorism, low set and posteriorly rotated ears, palatal abnormalities, micrognathia. Developmental delay, hypoplastic thymus, hypocalcaemia, variety of immunological abnormalities |
Allagile | JAG-1, NOTCH-2, dominant trait | Peripheral pulmonary stenosis | Facial dysmorphias (triangular face, wide nasal bridge, deep set eyes), intrahepatic cholestasis, butterfly vertebrae |
Keutel | MGP mutations, autosomal recessive trait | Multiple peripheral pulmonary stenosis | Abnormal cartilage calcifications, brachytelephalangy. subnormal IQ, hearing loss |
Congenital rubella | - | Peripheral pulmonary stenosis, open ductus Botalli | Congenital cataract/glaucoma, deafness, pigmentary retinopathy |
ASD, atrial septal defect; VSD, ventricular septal defect.
# Valvular Pulmonary Stenosis (PS) 瓣膜性肺动脉狭窄
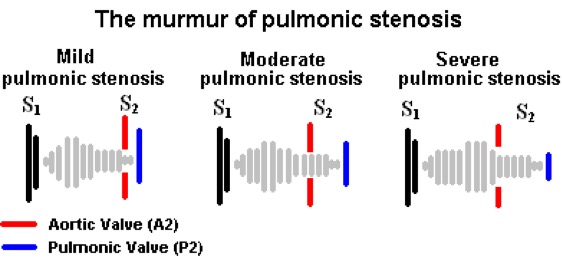
- Frequently asymptomatic systolic murmur
频繁无症状收缩期杂音
第二心音由主动脉瓣、肺动脉瓣关闭产生,如果存在狭窄,瓣膜关闭时间会延长,临床上表现为第二心音延长 - Mild PS seldom progresses; seldom symptomatic (ie no reduction in exercise tolerance)
轻度 PS 很少进展;很少有症状 (即运动耐力没有降低) - Moderate PS progressive; associated with RV hypertrophy
中度进行性 PS;与右室肥厚相关
如果实际操作中测得 PS 为轻度,应在多个切面放置 CW 或 PW,以反复确认跨瓣压差,避免低估狭窄程度 - Severe PS: exercise intolerance, dyspnoea, lightheadedness, chest pain (RV angina)
重度 PS,有临床症状:运动不耐受、腹泻、头晕、胸痛(右心室心绞痛)
右室提供了左室的血供,如果因为肺动脉瓣狭窄导致左室前负荷降低,充盈的延迟或减少,会导致血压降低导致头昏;如果有右室肥厚,血液必须供应更大量的肌肉,因此可能会出现心肌缺血(ischemia)而出现心绞痛症状
- Almost always congenital in origin; isolated valvular PS ~ 8-10% of all congenital heart defects
几乎都是先天性的;单纯瓣膜 PS 占所有先天性心脏病的 8-10% - Often associated with other complex congenital HD: eg ToF
常与其他复杂的先天性心脏病有关:例如法洛四联症 - Acquired PS: commonest is carcinoid (PS and PR), very rarely rheumatic
获得性 PS:最常见的是类癌 (肺动脉狭窄和反流),很少是风湿性的 - Congenital PS: dysplastic leaflets: ~ 20%
先天性 PS:瓣叶发育异常约占 20%
# SUB Valvular 瓣膜下
- Congenital: associated with VSD / ToF
先天性:与室间隔缺损 / 法洛四联症相关 - Acquired: due to severe RVH, prior surgery, associated with hypertrophic/infiltrative cardiomyopathy
获得性:由于严重的右室肥厚,既往手术,与肥厚性 / 浸润性心肌病相关 - Often PV is normal
通常情况下,肺瓣本身是正常的
# SUPRA Valvular 瓣膜上
- main pulmonary arteries(MPA), bifurcation, branch vessels
大肺动脉、分叉、分支血管 - Associated with Noonan's syndrome, Williams syndrome
与努南综合征、威廉姆斯综合征相关


# Pulmonary Regurgitation (PR) 肺动脉瓣反流
- Presents to some degree in 40-78% of individuals with normal pulmonary valves
40%-78% 的正常肺动脉瓣患者可有不同程度的反流表现 - Acquired PR due to dilatation of the PA: most commonly due to PHTN
由于 PA 扩张而获得的 PR:最常见的原因是 PHTN(肺动脉高压) - Severe PR usually Occurs with other cardiac abnormalities
严重的 PR 通常与其他心脏异常一起发生
# AETIOLOGY 病因学
- Congenital abnormalities: bicuspid/quadricuspid valve
先天性畸形:二尖瓣 / 四尖瓣 - Pulmonary valve hypoplasia 肺动脉瓣发育不全
- Post TOF repair 法洛四联症修复后
- Prolapse: rare 脱垂:罕见
- Bacteria endocarditis 细菌心内膜炎
- Carcinoid syndrome 类癌综合征
- Post valvotomy 瓣膜切开术后
# Echocardiographic evaluation 超声心动图评估
TTE, TOE, 3DE views (standard and modiffied)
标准和改良的切面- Limited visualisation; most difficult valve to evaluate
有限的可视化;视野受限,是最难评估的瓣膜 - Anomalies of the leaflet: no of cusps, thickening, doming, calcification
瓣叶形态异常:无尖、增厚、隆起、钙化
评估包括狭窄和反流(定性和定量) - Abnormal structure: hypoplasia, dysplasia
结构异常:发育不全、发育异常
- Limited visualisation; most difficult valve to evaluate
Evaluation of the PV should be performed in conjunction
应联合进行- RVOT 右室流出道
- RV 右室
- Pulmonary branches 肺动脉分支
- 狭窄时可能有 RVOT 扩张,右室肥厚
- 肺动脉主干或者分支有没有扩张,来评估狭窄的位置是瓣上还是瓣膜本身还是瓣下

- 左侧 9 点钟位置 —— 右房
- 上方 12 点钟位置 —— 右室
- 两者之间是三尖瓣
- 右下方 3 点钟位置 —— 肺动脉瓣、肺动脉主干,下方是两个肺动脉分支
# TTE





- PLAX, PSAX, Subcostal views
左侧胸骨旁(最常用)长轴、短轴,剑突下 - PSAX, standard view for assessment of the PV
胸骨旁短轴,是 PV 评估的标准视图 - Transducer position at base of heart where PA bifurcates
换能器放在心底部 PA 分叉处 - 患者左侧卧位,手放在头部后方
- 探头从胸骨旁长轴切面开始,顺时针 90° 旋转得到主动脉瓣水平短轴切面
- 向上向右肩倾斜,得到改良版的肺动脉瓣水平切面

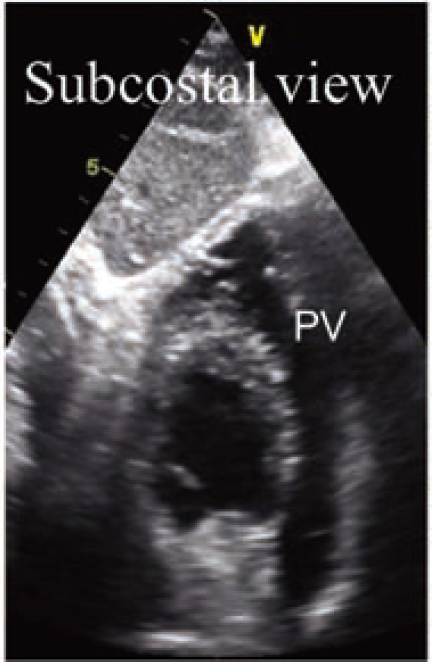
- Subcostal views with anterior angulation
剑突下切面伴探头前倾,成像角度不一样但内容与胸骨旁差不多- Transducer on abdomen just below xyphoid process
腹部剑突正下方的换能器 - Notch at 6 o'clock
切口指向 6 点钟位置 - Tilt the ultrasound probe leftward
向左倾斜超声探头
- Transducer on abdomen just below xyphoid process
# Pulmonary Valve (PV)
Qualitative to identify mechanism | Quantitative |
|---|---|
|
|
# Pulmonary Stenosis (PS)
- 2D Echo (anatomy and structure) 解剖与结构
- PLAX
- PSAX: level of the AV
- Thickened leaflets, doming, calcification
描述瓣叶,增厚、穹隆样改变、钙化 - Variable degree of commissural fusion
不同程度的交界区融合 - Post stenotic dilatation of MPA
狭窄后,肺动脉主干的继发扩张 - RV size is usually normal: as with RVH (>5mm) and RV hypoplasia
右室大小通常是正常的:例如伴右室肥厚 (>5 mm) 和右室发育不良
居中的是主动脉瓣,大概 1-2 点钟方向是肺动脉瓣。PV 看起来有点增厚、钙化,不像正常时的那么薄,有点穹隆样改变,活动有点僵硬,尤其是上方的瓣膜活动度欠佳。右方的肺动脉呈现瓣膜狭窄后继发的扩张(正常应该是小于主动脉部分的尺寸)。
看到这样的 2D 图像时,就应该要放上彩色血流、CW、PW 进行分析。


Echocardiographic measurements of right ventricular dimensions. (A) Parasternal long axis view. (B) Parasternal short axis view. (C) Apical four chamber view. Ao, aorta; LA, left atrium; LV, left ventricle; PA, pulmonary artery; RA, right atrium; RV, right ventricle; RVIT, right ventricular inflow tract; RVLAX, right ventricular long axis; RVOT, right ventricular outflow tract.
超声心动图测量右室内径。(A) 胸骨旁长轴观。(B) 胸骨旁短轴切面。(C) 心尖四腔切面。AO,主动脉;LA,左房;LV,左室;PA,肺动脉;RA,右房;RV,右室;RVIT,右室流入道;RVLAX,右室长轴;RVOT,右室流出道。
- Colour Flow Doppler 彩色血流
- Turbulence/aliasing 有无湍流 / 混叠现象
- Site of turbulence helps placement of Doppler cursor 湍流位置及方向有助于放置多普勒取样线,进行最大血流速度的描绘
- Associated regurgitation 伴反流
在 2D 下如果见到了肺动脉瓣增厚或穹隆样改变,可以加上彩色血流。彩色血流图可以看到湍流,在放置 CW 或者 PW 时,可以使取样线对齐湍流的方向,以获得最大速度来确定狭窄的程度
舒张期也可以观察有没有肺动脉瓣反流,若存在,也需要评估和分析
- Doppler PW and CW
- PW Doppler
- locate the site of peak velocity
定位峰值速度的位置
- locate the site of peak velocity
- CW Doppler
- Peak velocity/VTI
峰值速度 / 速度时间积分 - Mean gradient
平均压差 - Peak gradient (4V2)
峰值压差
- Peak velocity/VTI
- 3-5 cycles to adjust for respiratory changes
3-5 个周期以适应呼吸变化
- PW Doppler


完整超声评估一般开始于胸骨旁长轴,进行成像,观察室间隔、左室内腔、下侧壁或使用 2D M 型进行测量,然后是彩色多普勒,观察各瓣膜有没有湍流或反流
左室长轴结束后,切到右室流入道流出道观察。右室流出道包括右室流出道、肺动脉瓣、肺动脉主干的观察。
再到胸骨旁短轴切面,成像主动脉瓣水平以及改良版看肺动脉瓣,加持彩色多普勒,若存在异常可以 CW 或 PW 进行定量分析
继续进行心尖四腔五腔三腔等系统的完整评估
| Mild | Moderate | Severe | ||
|---|---|---|---|---|
| CW | Peak Doppler velocity (m/s) 最大速度 | <3 | 3-4 | >4 |
| Peak Doppler gradient (mmHg) 最大跨瓣压差 | <36 | 36- 64 | >64 | |
| Mean Doppler gradient (mmHg) 平均跨瓣压差 | > 40 |
- Aways check tricuspid regurgitation gradient to rule out overestimation of pulmonary stenosis gradient
通常也要评估三尖瓣反流压差,以避免高估肺动脉狭窄程度
# Supravalvular PS
- Often associated with syndromes 通常伴有综合征的出现
- Can have stenosis at multiple sites ie MPA + branched PA
狭窄可以出现在多个部位(例如主干 + 分支或更远端) - PV gradient should comprise most of RVSP if single for stenosis
如果狭窄是单一的,跨肺动脉瓣压差应该包括大部分右室收缩压


- CW 应该尽量取样到合适的部位以获得最大血流速度,以更好的估算压差
# Pulmonary Regurgitation (PR)
- Diastolic jet in the RVOT 右室流出道中的舒张期血流
- Jet length >10 mm 射流长度 > 10 毫米
- Physiological vs pathological PR: duration of flow ie holodiastolic
生理与病理 PR: 血流持续时间,即全舒张期 - Jet width: wider jets worse; evaluate at jet origin "vena contracta" [2]
射流宽度:较宽的射流更糟;在反流起始处评估缩流颈宽度 - Severe PR: jet width vs RVOT width > 55-65%
严重 PR: 射流宽度 vs RVOT 宽度 > 55-65% - Detection of flow reversal in pulmonary arteries
肺动脉血流逆转的检测
 and regurgitant jet width in two patients with TR. Bottom: continuous wave Doppler recordings.")

- CW Doppler: jet intensity (qualitative)
连续波多普勒:反流束强度 (定性) - Rapid flow deceleration (short PHT < 100ms)
血流快速减速 (短 PHT<100ms)

- (A) left, complete lack of valve coaptation and right, the measurement of the vena contracta width(VC);
- (B) colour-coded M-mode depicting the time-dependency of flow signal during the heart cycle;
- (C) continuous Doppler recording of PR showing a rapid flow deceleration during the diastole (red arrow) and increased systolic flow velocity (not related to concomitant pulmonary stenosis).
PR 的连续多普勒记录显示舒张期血流迅速减速 (红色箭头),收缩期血流速度增加 (与合并的肺动脉狭窄无关)。

- CW Doppler of pulmonic flow. Calculation of pulmonic regurgitation index (PR index = A/B) is shown, an index of PR severity, quantitating early termination of diastolic regurgitant flow.
肺动脉血流的连续波多普勒。计算了肺动脉反流指数 (PR 指数 = A/B,A = 反流时长,B = 反流开始到肺动脉瓣再次打开),作为 PR 严重程度的指标,量化了舒张期反流束的早期终止。
| Pulmonary regurgitation | |||
|---|---|---|---|
| Mild | Moderate | Severe | |
| Pulmonic valve 肺动脉瓣形态 | Normal | Normal or abnormal | Abnormal and may not be visible |
Right ventricle (Size) 右室大小 | Normal1 | Normal or dilated | Dilated2 |
RegJetlength 反流束长度
| Thin with a narrow origin 稀薄、起源窄 | Intermediate | Broad origin; variable depth of penetration |
RatioRegJet/PV 反流束宽度与瓣环径比值
| > 70%3 | ||
RegJetdensity 反流束密度(CW)
| Soft | Dense | Dense; early termination of diastolic flow |
DTRegJet 反流束减速时间
| Short4 短 | ||
PHTRegJet 反流束压差减半时间
| < 100ms5 | ||
PR index6 肺动脉瓣反流指数
| < 0,77 | < 0,77 | |
PAreversal flow 肺动脉逆向血流
| Yes | ||
PV VTI / LVOT VTI7 肺瓣 VTI 与左室流出道 VTI 之比
| Slightly increased | Intermediate | Greatly increased |
RF8 肺动脉瓣反流分数
| < 20% | 20-40% | > 40% |
- Unless there are other reasons for RV enlargement.
除非有其他原因导致 RV 扩大。 - Exception: acute PR. 排除急性反流
- Identifies a CMR-derived PR fraction > 40%.
确定 CMR 所测得的 PR 分数 > 40%。 - Steep deceleration is not specific for severe PR.
陡峭减速不是严重 PR 所特有的 - Not reliable in the presence of high RV end diastolic pressure.
在存在高 RV 舒张末期压力的情况下不可靠 - Defined as the duration of the PR signal divided by the total duration of diastole, with this cutoff identifying a CMR-derived PR fraction > 25%.
定义为 PR 信号的持续时间除以舒张期的总持续时间,该分界值识别 CMR 所测得 PR 分数 > 25%。 - Cutoff values for regurgitant volume and fraction are not well validated.
反流体积和分数的分界值没有得到很好的验证 - RF data primarily derived from CMR with limited application with echocardiography.
反流分数的数据主要来自 CMR,超声心动图的应用有限。
Other techniques of PR quantification
- Very limited data; small sample size and not validated
数据非常有限;样本量小,未经验证
- PW Doppler: $$ \text{difference between reverse and forward VTI} = \% \text{regurgitant flow} $$
PW 多普勒:反向与正向 VTI 的差值 = 反流血流的百分比- PV forward VTI vs AV forward VTI < 1 normally
正常情况下,PV 正向 VTI 与 AV 正向 VTI 之比 < 1- Not validated; no ref ranges
未验证;没有参考范围
- EROA (mm2)
- PISA method
Cuypers, J. A. A. E., Witsenburg, M., van der Linde, D. & Roos-Hesselink, J. W. Pulmonary stenosis: update on diagnosis and therapeutic options. Heart 99, 339–347 (2013). ↩︎
Lancellotti, P. et al. Recommendations for the echocardiographic assessment of native valvular regurgitation: an executive summary from the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 14, 611–644 (2013). ↩︎