# Learning objectives
- Definition 定义
- Diagnosis 诊断
- Diagnostic echocardiography criteria 超声诊断标准
- Echocardiographic estimation of outcome 超声对预后的评估
- Intracardiac complications of endocarditis 心内膜炎的心内并发症
- Prosthetic valve endocarditis 人工瓣膜心内膜炎
- Treatment: Medical and surgical 治疗:药物和手术
# Definition
- Infection of the endocardial surface of the heart characterised by:
心脏心内膜表面感染的特征是:- Colonisation or invasion of the heart valves (native or prosthetic) or the mural endocardium by a microbe
微生物对心脏瓣膜 (天然的或人工的) 或心内膜的定植或侵入 - Leading to formation of bulky, friable vegetation composed of thrombotic debris and organisms
导致形成由血栓碎片和生物体组成的笨重、易碎的赘生物 - Often associated with destruction of underlying cardiac tissue.
通常与潜在心脏组织的破坏有关
- Colonisation or invasion of the heart valves (native or prosthetic) or the mural endocardium by a microbe
# Background
- A rare disease with an increase incidence up to 11 episodes/100 000 persons a year
一种罕见疾病,发病率每年增加 11 次 / 10 万人 - High mortality disease: 15-30% 高死亡率疾病
- Poor prognosis 预后不良
- The diagnosis remains difficult 诊断仍然很困难
# Epidemiology 流行病学
- An increase in incidence
发病率增加 - Older patients 老年患者
- Shift from streptococci to staphylococci 从链球菌转移到葡萄球菌
- Without any history of valvular disease (53% of patients with IE). 没有任何瓣膜疾病史(占 IE 患者的 53%)。
# Diagnosis 诊断
# Duke Criteria Duke 标准
# Major criteria
Positive blood culture 血培养阳性
- Typical organism from two cultures 两种典型菌
- Persistent positive blood cultures taken > 12hrs apart
间隔 > 12 小时持续 - Three or more positive cultures taken over > 1hr
三种或三种以上血培养阳性时间超过 1 小时
Endocardial involvement 心内膜受累
- Positive echocardiographic findings of vegetations
超声心动图赘生物阳性结果 - New valvular regurgitation
新出现的瓣膜返流
- Positive echocardiographic findings of vegetations
# Minor criteria
- Predisposing valvular or cardiac abnormality
易感瓣膜或心脏异常 - Intravenous drug misuse
滥用静脉药物 - Pyrexia ≥ 38 °C 高热
- Embolic phenomenon 栓塞现象
- Vasculitic phenomenon 血管炎现象
- Blood cultures suggestive: organism grown but not achieving major criteria
血液培养提示:细菌生长但未达到主要标准 - Suggestive echocardiographic findings
超声心动图有所发现
# Duke Criteria
1994 a group at Duke University standardised criteria for assessing patients with suspected endocarditis
Definite 确诊
- 2 major criteria
- 1 major and 3 minor criteria
-5 minor criteria - pathology/histology findings 病理学 / 组织学发现
Possible 可能
- 1 major and 1 minor criteria
- 3 minor criteria
Rejected 排除
- firm alternate diagnosis 明确的替代诊断
- resolution of manifestations of IE with 4 days antimicrobial therapy or less
用 4 天或更短的抗菌治疗即可消除 IE 症状
# Clinical features
- Regurgitation murmur 反流杂音(新出现的)
- Vascular symptoms 脉管症状
- Immune symptoms 免疫症状

- Minor criteria
- Predisposition such as predisposing heart condition, or injection drug use.
易感因素,如易患心脏病或注射药物。 - Fever defined as temperature >38°C.
发烧定义为体温 - Vascular phenomena (including those detected by imaging only): major arterial emboli, septic pulmonary infarcts, infectious (mycotic) aneurysm, intracranial haemorrhage, conjunctival haemorrhages, and Janeway's lesions.
血管现象(包括仅通过影像检查发现的血管现象):主要动脉血栓、感染性肺梗塞、感染性(真菌性)动脉瘤、颅内出血、结膜出血和 Janeway 病变。 - Immunological phenomena: glomerulonephritis, Osler's nodes, Roths spots, and rheumatoid factor
免疫学现象:肾小球肾炎,奥斯勒氏结节,罗斯斑点和类风湿因子 - Microbiological evidence: positive blood culture but does not meet a major criterion as noted above or serological evidence of active infection with organism consistent with IE.
微生物学证据:血液培养呈阳性,但不符合上述主要标准,或血清学证据表明与 IE 一致的病原菌存在活动感染。
- Predisposition such as predisposing heart condition, or injection drug use.
# Typical organisms: Blood culture
- Microbiology of Infective Endocarditis. [1]
感染性心内膜炎的微生物学
| Streptococcaceae 链球菌 | 240 (48%) |
| Oral streptococci 口腔链球菌 | 93 (19%) |
| Group D streptococci D 群链球菌 | 62 (13%) |
| Pyogenic streptococci 化脓性链球菌 | 25 (5%) |
| Enterococci 肠球菌 | 52 (10%) |
| Other Streptococcaceae 其他链球菌 | 8 (2%) |
| Staphylococcaceae 葡萄球菌 | 180 (36%) |
| Staphylococcus aureus 金黄色葡萄球菌 | 132 (27%) |
| Other microorganisms 其他微生物 | 42 (9%) |
| ≥ 2 microorganisms 合并两种微生物 | 9 (2%) |
| None identified 未明确 | 26 (5%) |
- Increased prevalence of staphylococci IE
葡萄球菌 IE 患病率上升


# Imaging
TTE and TOE are the first line imaging for the diagnosis of IE
TTE 和 TOE 是诊断 IE 的一线影像学检查Limitations of TTE: 经胸超声的局限性
- Underestimates size and complexity of large vegetations
低估了大型赘生物的大小和复杂性 - May fail to detect small vegetations(< 3 mm).
可能无法检测到微小的赘生物 (<3 毫米)。
- Underestimates size and complexity of large vegetations
Goals of Echo in IE: 超声目标
- Identify, localise and characterise masses consistent with vegetation
识别、定位和描述与赘生物一致的团块 - Identify new valvular regurgitation
确定到有新的瓣膜反流 - Examine prosthetic valve stability
检查人工瓣膜的稳定性 - Apply criteria to judge prognosis once vegetation identified.
一旦发现赘生物,应用测量尺寸等标准来判断预后。
- Identify, localise and characterise masses consistent with vegetation
# Accuracy of Imaging
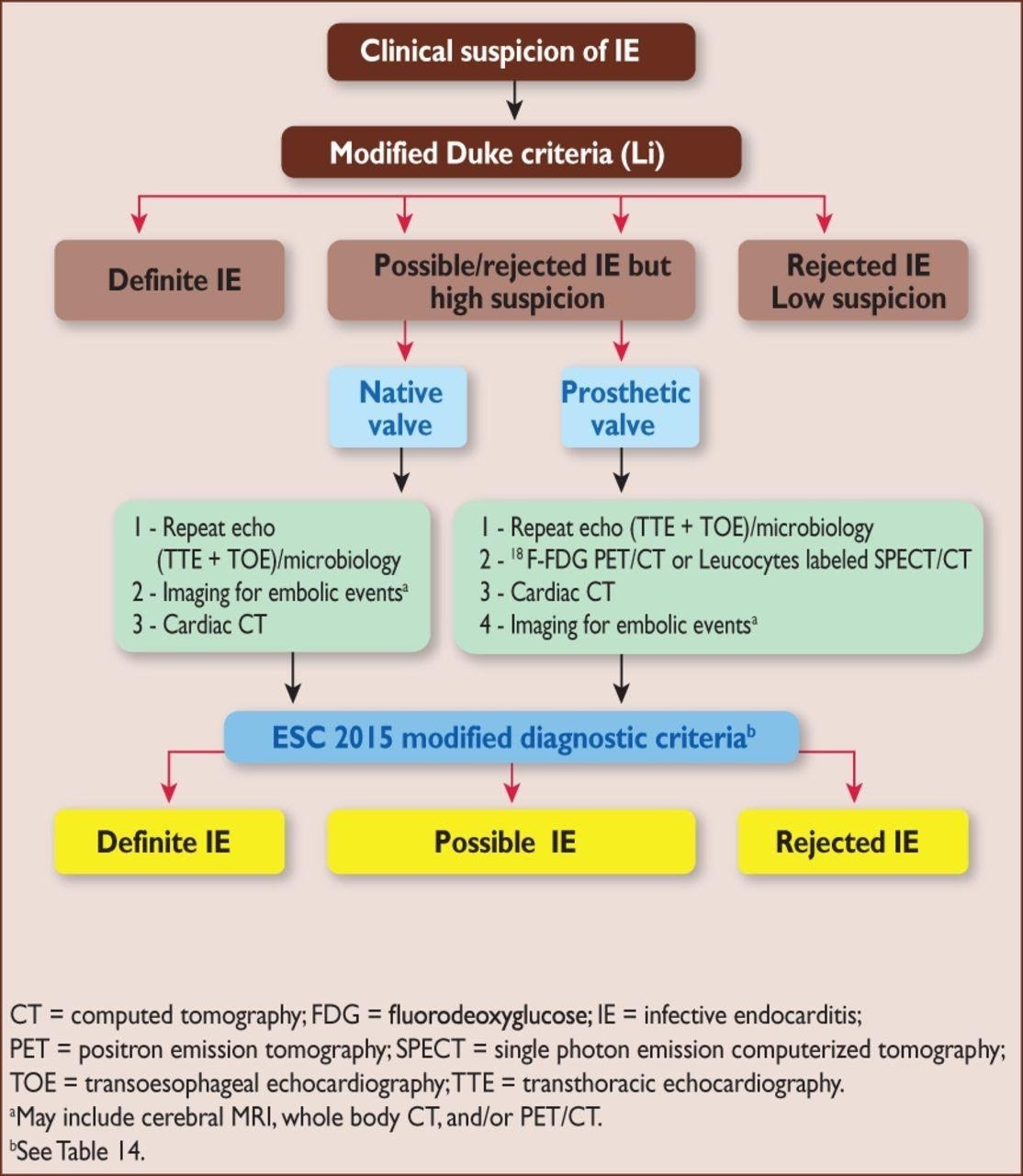
- Sensitivity = 70% for native valve and 50% for prosthetic valve with TTE, and 96% and 92% for TOE [2]
敏感性 - TTE 自体瓣膜 70%,人工瓣膜 50%,TOE 分版为 96% 和 92% - Specificity = 90% for both TTE and TOE
特异性 - 均为 90% - BUT NOT 100%.
可能需要其他手段,比如 PET/CT;脑补 MR 看有没有脑梗的表现
# Diagnostic Echo Criteria 诊断超声标准
- Characteristics of mass likely to be vegetation:
团块可能是赘生物的特征:- Texture: Grey scale and reflectance of myocardium
纹理:类似心肌的灰度和反射率 - Location: Upstream side of valve in path of jet or on prosthetic material
位置:射流路径或人工瓣膜的上游侧 - Motion: Chaotic and orbiting, independent of valve motion
活动度:混沌和轨道运动,与瓣膜运动无关- Prolapse into upstream chamber (i.e. MV mass into LA in systole
脱垂进入上游腔室 (例如收缩期进入 LA 的 MV 团块;主动脉瓣的赘生物一般长在左室侧,如果足够的长有可能在收缩期进入主动脉,舒张期再进入左室)
- Prolapse into upstream chamber (i.e. MV mass into LA in systole
- Shape: Lobulated, amorphous
形状:叶片状,无固定形态 - Accompanying abnormalities: 伴随异常
- Abscess, fistula, new regurgitant lesion, paravalvular leak.
脓肿、瘘管、新的反流性病变、瓣周漏。
- Abscess, fistula, new regurgitant lesion, paravalvular leak.
- Texture: Grey scale and reflectance of myocardium

- Characteristics of mass Inlikely to be vegetation:
不太可能是赘生物的团块特征:- Texture: Reflectance myocardium or pericardium (white)
纹理:高于心肌或心包的亮度 (白色) - Location: Outflow tract attachment, downstream surface of valve
位置:附着在流出道,瓣膜下游表面 - Shape: Stringy or hair-like strands with narrow attachment
形状:线状的或毛发状的,狭窄的附着物 - Lack of accompanying turbulent flow or regurgitation.
没有伴随的湍急流动或反流
- Texture: Reflectance myocardium or pericardium (white)

- False Positives 假阳性
- Most common on TEE 在 TEE 上最常见的
- Lambl's excrescences Lambl 赘生物
- Strands on sewing rings of prosthetics
假体瓣膜缝纫环上的线 - Free suture 游离缝合线
- Redundant chordae 多余的腱索
- Chiari's remnant in RA 残留在 RA 的 Chiari 网
- All of above tend to be highly reflective with echodensity similar to pericardiun Or aortic root. Dense, fibrotic and non-vibratoi
以上所有这些都具有高度反射性,回声密度类似于心包或主动脉根部。致密、纤维化且无振动

- False Negatives 假阴性
- TTE > TOE
- High sensitivity of TOE (92-94%)
经食道超声灵敏度更高 - Cannot definitively rule out endocarditis
不能明确排除心内膜炎 - Low likelihood of IE, if negative TOE in intermediate probability patient
如果中危患者 TOE 检查为阴性,发生 IE 的可能性低 - In patients at high risk for IE (prosthetic valve, unexplained bacteraemia), repeat examination reasonable.
对于 IE 高危患者(有假体瓣膜、不明原因的菌血症),重复检查是合理的。
# Multimodality imaging 多模态成像
CT Scan
- Diagnosis (vegetation, abscess, pseudoaneurysm)
诊断(赘生物、脓肿、假性动脉瘤) - Embolic lesions
栓塞性病变
- Diagnosis (vegetation, abscess, pseudoaneurysm)
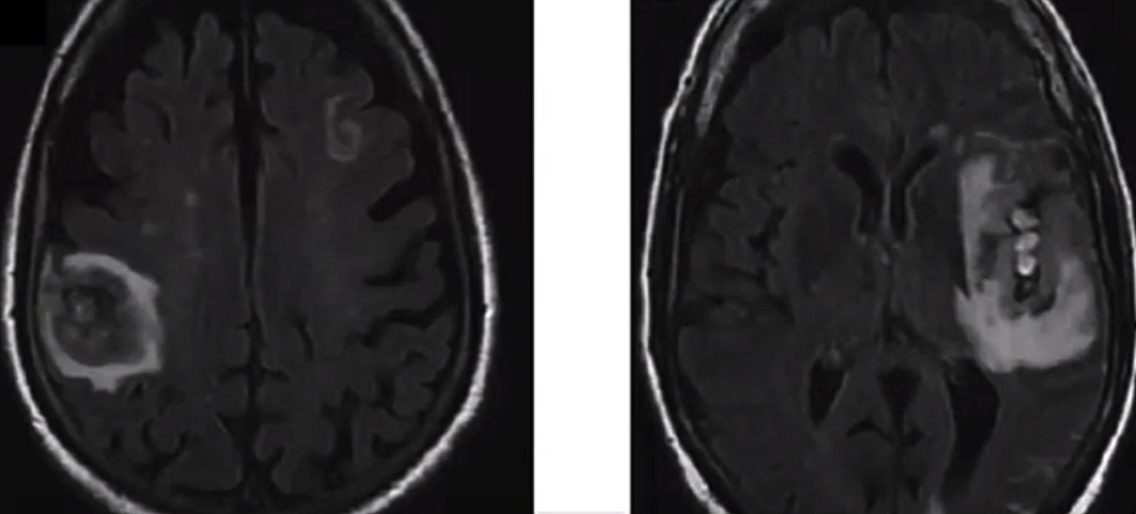
MRI
- Embolic lesions, especially cerebral complications.
栓塞性病变,尤其是脑部并发症
- Embolic lesions, especially cerebral complications.
PET CT scan
- Better sensitivity for the detection of prosthetic IE
假体瓣膜 IE 的检测灵敏度较高 - Sens 97%, Spec 80%.
- Better sensitivity for the detection of prosthetic IE
# Echo Estimation of Outcome 超声预估预后
- Size of vegetation most powerful predictor of Clinical complications (drug failure, new CHF, embolisation, surgery)
赘生物的大小是临床并发症 (药物失效、新发心力衰竭、栓塞、手术) 最有力的预测因素,因此一定要测赘生物的大小- 10% in 6 mm vegetation, 50% if 11 mm and almost 100% if 16 mm
6mm 的赘生物约 10% 发生,11mm 的赘生物则为 50%,16mm 的赘生物几乎 100%
- 10% in 6 mm vegetation, 50% if 11 mm and almost 100% if 16 mm
- Complication more frequent with higher grades of mobility and lesion extent
活动度越高,病变范围越大,并发症越多 - Vegetation consistency does not predict complications (except for calcifed lesions which has no associated complications)
赘生物的连贯性不能预测并发症(钙化病变除外,钙化病变没有相关并发症) - Echo predictors still apply after initiation of antibiotics.
在开始使用抗生素后,超声预测仍然适用。
# Intracardiac Complications 心内并发症
- Valvular regurgitation 瓣膜反流
![]()
- Secondary infection of other valves 其他瓣膜继发感染
- Leaflet perforation 瓣叶穿孔,穿孔个数
- Perivalvulal abscess or fistula: 瓣周脓肿或瘘管
- Abscess most likely with staph aureus 脓肿很可能与金黄色葡萄球菌有关
- Abscess formation --> increase in morbidity and mortality.
脓肿形成 --> 发病率和死亡率增加
# Right Sided Endocarditis 右侧心内膜炎
Tricuspid valve vegetation most common in IV drug users
三尖瓣赘生物最常见于静脉药物成瘾者Mostly caused by staph aureus
多由金黄色葡萄球菌引起Pacemaker Associated Endocarditis 起搏器相关性心内膜炎
- More leads than ever being placed
导线放置过多 - Symptoms are vague - mimic pneumonia
症状模糊,类似肺炎 - Look for vegetations along wires
沿着导线寻找赘生物 - Vegetations are mobile
赘生物是可移动的 - Thrombus and masses may look similar
血栓和肿块可能看起来很相似 - Treatment: Abx, removal, variable
治疗:抗生素,去除,可变
- More leads than ever being placed
# Prosthetic Valve Endocarditis 人工瓣膜心内膜炎
- Findings suggestive of IE in prosthetic valves:
发现人工瓣膜中存在 IE:- Vegetation 赘生物
- Valve rocking suggesting valve dehiscence
瓣膜摇晃提示瓣膜裂开 - Perivalvular regurgitation/abscess
瓣周反流 / 脓肿 - Impaired leaflet motion
瓣叶运动受损 - Must compare to prior
必须与之前进行比较
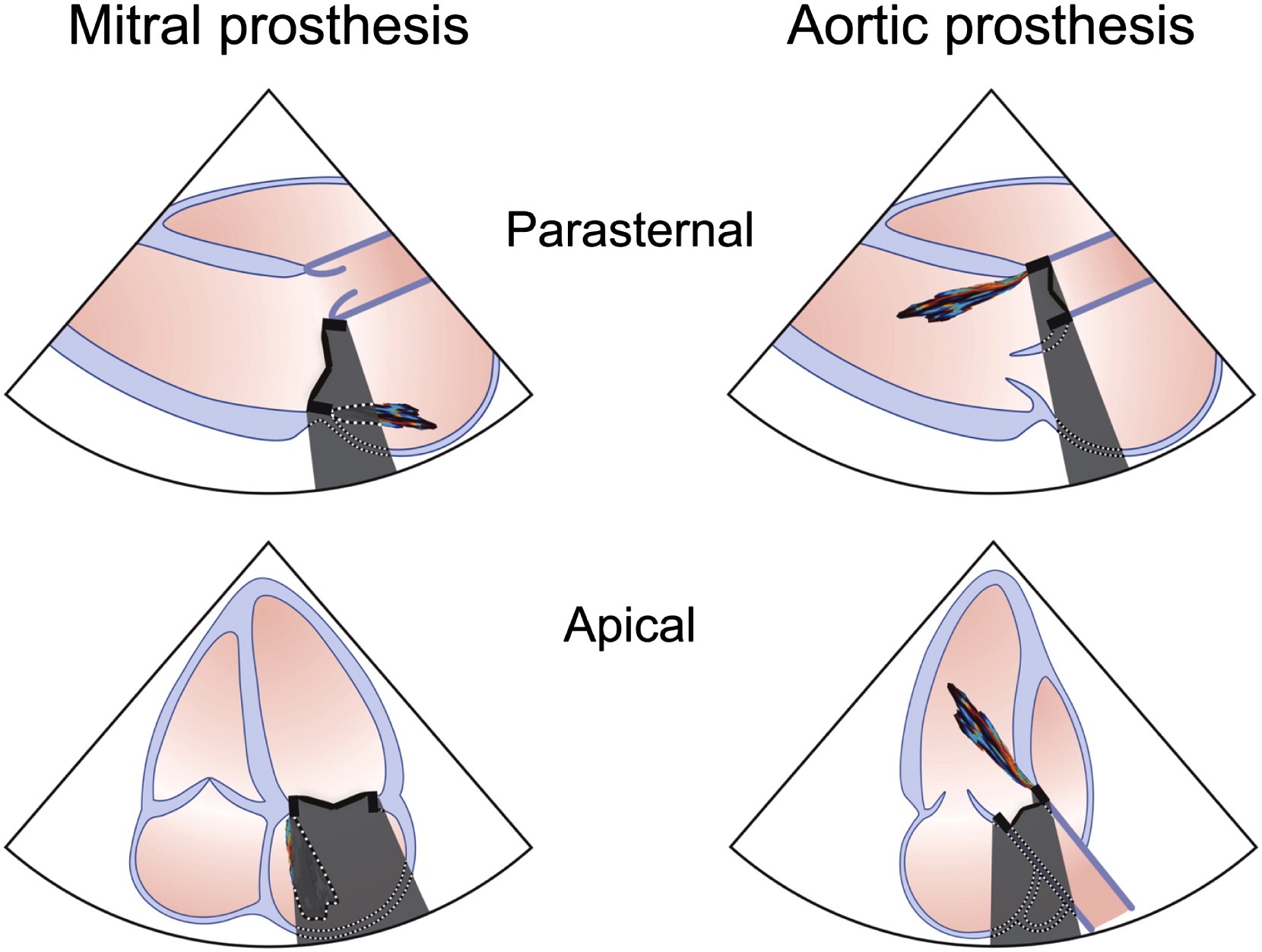
- Echo evaluation limited prosthetic shadow
回声评估有限由于假体阴影 - Low threshold to use TOE.
经食道超声使用低阈值
# Management 管理
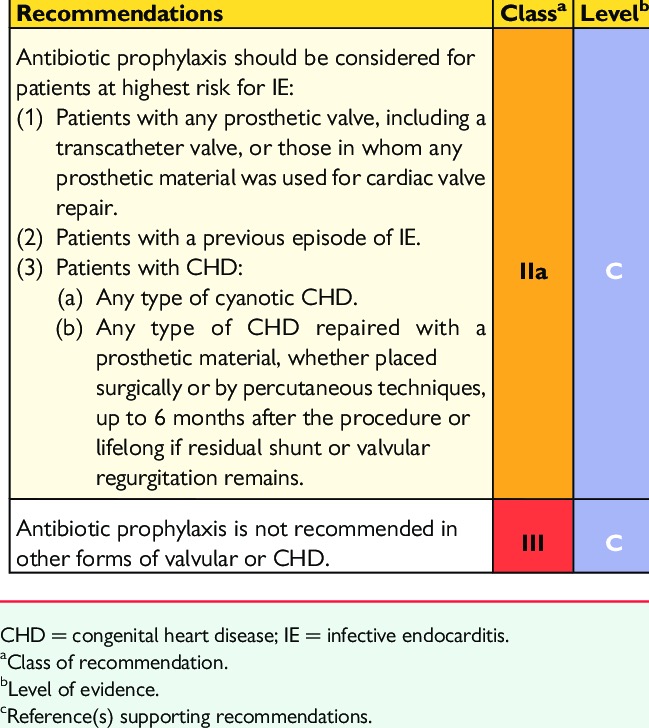
# Prophylaxis 预防
Only for patients at highest risk of IE
仅适用于 IE 风险最高的患者![]()
Antibiotic prophylaxis for dental procedures requiring manipulation of the gingival tissue or perforation of the oral mucosa
用于需要操作牙龈组织或口腔粘膜穿孔的牙科手术的抗生素预防,Antibiotic: Amoxicillin or ampicillin if no allergy, clindamycin if allergy.
抗生素:如果没有过敏,选择阿莫西林或氨苄西林,如果过敏,选择克林霉素。
# Surgery
Surgery: To prevent or treat life threatening complications
预防或治疗危及生命的并发症- Heart failure (30-40%) due to acute valve regurgitation
急性瓣膜反流引起的心力衰竭 (30-40%)- Reduced mortality after surgery
术后死亡率降低
- Reduced mortality after surgery
- Heart failure (30-40%) due to acute valve regurgitation
Systemic embolism (20% with clinical manifestations)
系全身性栓塞(20% 有临床表现)Uncontrolled infection (10-20% 不受控制的感染
- Higher mortality, higher rate of complications (conduction disorder, peri operative mortality, need of a second surgery).
更高的死亡率,更高的并发症发生率 (传导障碍,围手术期死亡率,需要第二次手术)。
- Higher mortality, higher rate of complications (conduction disorder, peri operative mortality, need of a second surgery).
Indications and Timing of Surgery [2:1]
左侧瓣膜感染性心内膜炎 (自体瓣膜心内膜炎和人工瓣膜心内膜炎) 的手术适应症和手术时机")
- HACEK = Haemophilus parainfluenzae, Haemophilus aphrophilus, Haemophilus paraphrophilus, Haemophilus influenzae, Actinobacillus actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, Kingella kingae and Kingella denitrificans; HF = heart failure; IE = infective endocarditis; NVE = native valve endocarditis; PVE = prosthetic valve endocarditis.
HACEK = 副流感嗜血杆菌、嗜人嗜血杆菌、副嗜血杆菌、流感嗜血杆菌、伴生放线杆菌、人心脏杆菌、腐蚀性艾肯氏杆菌、金黄色葡萄球菌和脱氮金黄色葡萄球菌;HF = 心力衰竭;IE = 感染性心内膜炎;NVE = 自体瓣膜心内膜炎;PVE = 人工瓣膜心内膜炎。 - a, Emergency surgery: surgery performed within 24 h; urgent surgery: within a few days; elective surgery: after at least 1–2 weeks of antibiotic therapy.
急诊手术:24 小时内手术;紧急手术:几天内;择期手术:抗生素治疗至少 1-2 周后。 - b, Class of recommendation.
- c, Level of evidence.
- d, Reference(s) supporting recommendations.
- e, Surgery may be preferred if a procedure preserving the native valve is feasible.
如果保存原生瓣膜的程序可行,手术可能是首选。
- HACEK = Haemophilus parainfluenzae, Haemophilus aphrophilus, Haemophilus paraphrophilus, Haemophilus influenzae, Actinobacillus actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, Kingella kingae and Kingella denitrificans; HF = heart failure; IE = infective endocarditis; NVE = native valve endocarditis; PVE = prosthetic valve endocarditis.
左侧瓣膜感染性心内膜炎 (自体瓣膜心内膜炎和人工瓣膜心内膜炎) 的手术适应症和手术时机")
# Infective Endocarditis TEAM
- IE is NOT a single disease
IE 不是一种单一的疾病 - High level of suspicious is needed
需要高度的可疑 - High level of expertise
高水平的专业知识 - Early discussion with surgery team
与外科团队进行早期讨论 - The prognosis depends on an early management
预后取决于早期治疗
Slipczuk, L., Codolosa, J. N., Davila, C. D., Romero-Corral, A., Yun, J., Pressman, G. S., & Figueredo, V. M. (2013). Infective endocarditis epidemiology over five decades: a systematic review. PloS one, 8(12), e82665. ↩︎
Habib, G., Lancellotti, P., Antunes, M. J., Bongiorni, M. G., Casalta, J. P., Del Zotti, F., ... & Zamorano, J. L. (2015). 2015 ESC guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European Society of Cardiology (ESC) endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). European heart journal, 36(44), 3075-3128. ↩︎ ↩︎