# Part 1 Question and Answers
The arrow here points to:
![]()
In a person with suspected paravalvular (mechanical) mitral regurgitation, the following transducer position has the best chance of revealing the mitral regurgitation jet:
对于怀疑为 (机械性) 二尖瓣瓣周漏的患者,下列探头位置最有可能显示二尖瓣反流:
机械二尖瓣会产生伪影,考虑这个因素,加持彩色多普勒时,胸骨旁长轴反流的声束会和这个伪影的方向刚好呈 90 度,可以更好的观察。如果是心尖四腔或两腔或长轴,刚好伪影是在下方的心房内,而反流束也在下方,会有一定的遮挡,不容易观察反流情况。
虽然考虑到伪影的情况,但是在实际临床操作中,要做完整的 TTE 记录图,每个切面都是要进行采集、分析和观察,只是 PLAX 最佳。The most common benign tumour in the heart is:
心脏中最常见的良性肿瘤是:
![]()
粘液瘤一般是连接于房间隔呈团块状的一个结构。
本图基本上是发生在瓣膜上的一个结构。
乳头状纤维弹性瘤可以成一个状的一个结构,有点有时类似于心内膜腱索的结构,它有这个心内膜的一些成分。
一般这种疾病的多见于患有心脏疾病的老年人。它是心脏最常见的一种良性肿瘤。The most common metastatic malignant tumour of the heart is:
心脏最常见的转移性恶性肿瘤是:
黑色素瘤一般始发于皮肤,有很强的向脑部还有心脏转移的特点。
The following are potential complications of aortic valve endocarditis:
以下是主动脉瓣心内膜炎的潜在并发症:
主动脉瓣感染性心膜炎是由细菌或者真菌感染引起的,导致主动脉瓣膜的破坏性改变,可以引起主动脉瓣反流,也可以引起主动脉根部的脓肿、漏管的形成。
Risk of aortic dissection is increased in the following conditions except:
除以下情况外,主动脉夹层的风险增加:
由于马凡氏综合症会引起主动脉根部的扩张。二叶式主动脉瓣会引起主动脉瘤的产生,以及孕期激素的改变、心脏血流的改变,都可以增加主动脉夹层的风险。
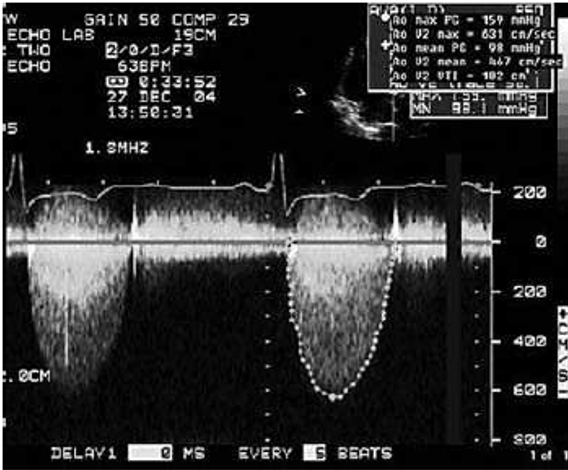
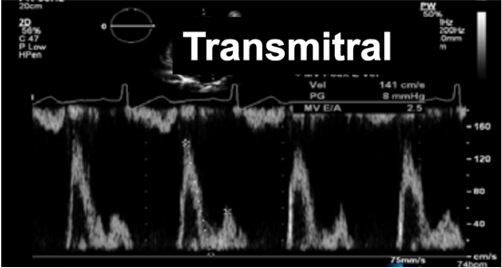
This patient is likely to have:
该患者可能患有:
![]()
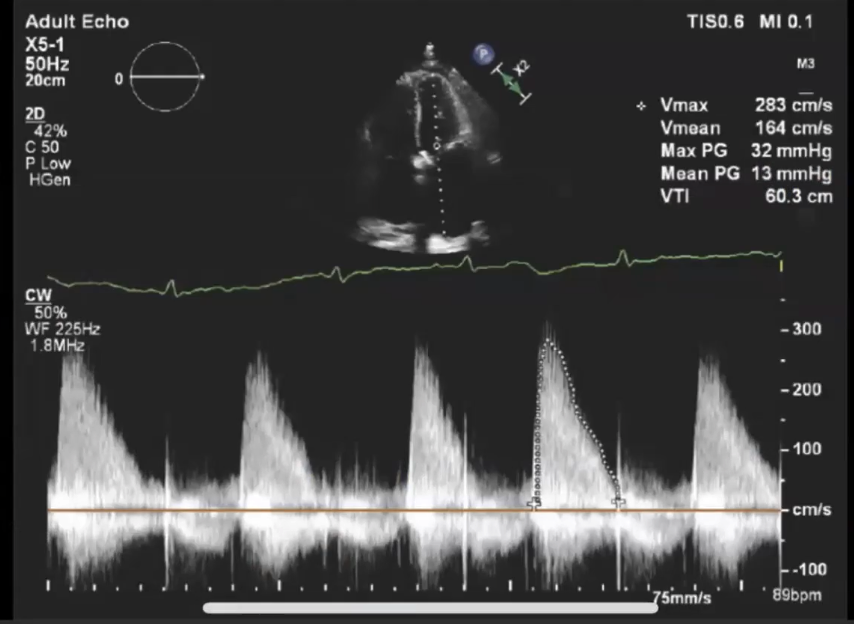
连续多普勒取样线放置在主动脉瓣而得到的频谱图,可以看到最大血流速度,根据右上角的提示,已经达到了 6.3 m/s,大于 4 m/s,是重度主动脉瓣狭窄的超声表现之一。
对于这个诊断,除了放置连续多普勒去测量最大血流速度、平均跨瓣压差,也可以根据连续方程式来计算瓣口面积,也可以根据周边的结构,比如有没有存在左室的肥厚等,一些会引起其他的心脏结构改变的线索,来综合的判断主动脉瓣狭窄的严重程度。Dilatation of the pulmonary artery is seen in all of the following conditions except?
肺动脉扩张在以下所有情况下都可以看到,除了?
房间隔缺损,一般存在左向右的大量分流,使右侧的容量负荷过高,可以引起肺动脉的扩张。
瓣膜性肺动脉狭窄和肺动脉高压由于存在狭窄,可以引起肺动脉的后扩张。
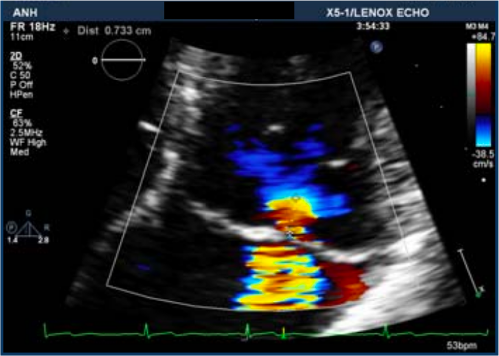
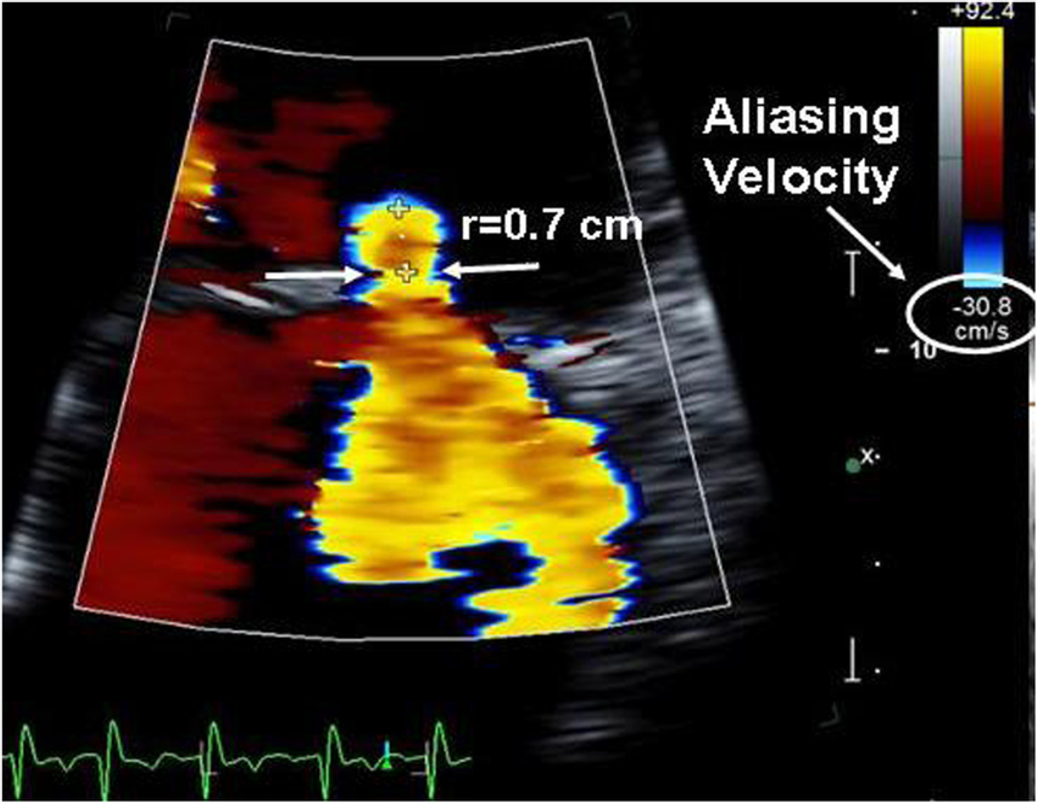
在临床上做 CT 冠脉造影时,可能有肺动脉呈扩张状态的报告,则需要寻找原因。大多是因为肺动脉高压,或者是左心疾病导致的继发性肺动脉高压。同时还需要进行心超检查,看有没有存在瓣膜水平的肺动脉狭窄,或其他导致肺动脉高压的原因,比如有没有存在房间隔缺损。The amount of tricuspid regurgitation in this patient is:
该患者的三尖瓣反流量为:
![]()
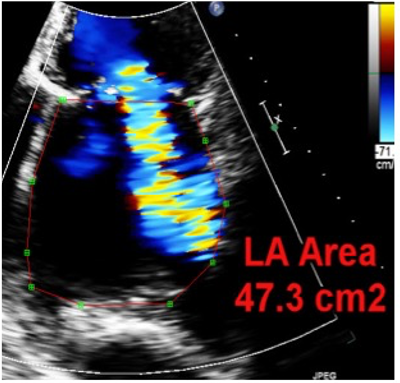
首先这是一个心尖四腔心切面,图片的左侧是患者的右心,可以看到右心室是显著扩张的,右心房也存在扩张。加上彩色血流多普勒后,可以看到有 TR,几乎充盈了整个右房(torrential)
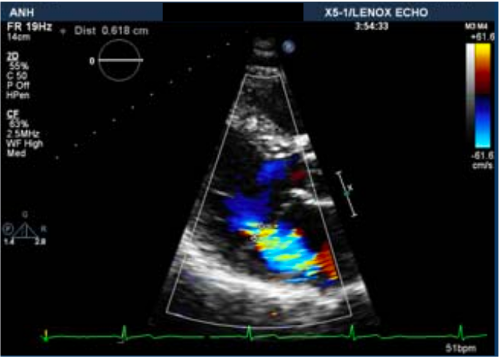
在正常人群中有可能出现轻度的三尖瓣反流,约 15% 的人有中度三尖瓣反流,但如果出现类似这样 torrential 的意味着重度,这是异常的。要对瓣膜本身的结构进行观察,寻找反流产生的原因。比如仔细观察 2d 超声,寻找原因。比如已知三尖瓣瓣叶很薄,是心内膜炎导致的瓣叶穿孔吗?还是右心室扩张还是右室心肌病,导致三尖瓣瓣环扩张,三尖瓣对合不良。The image of the aortic valve is suggestive of:
主动脉瓣的图像提示:
![]()
赘生物在左室流出道进出 Flopping,另一端 attached
根据诊断感染性心内膜炎的 Duke 标准,来综合判断The parasternal long axis image of the mitral valve apparatus show:
二尖瓣装置的胸骨旁长轴图像显示:
![]()
和瓣环钙化很难做鉴别。
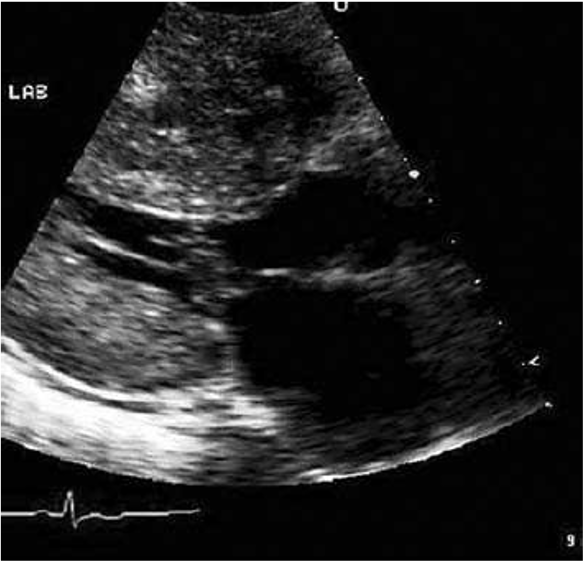
钙化的位置要比人工瓣环要低,且图中有人工瓣环的伪影The image shown here is suggestive of:
这里显示的图像暗示着
![]()
可以看到瓣架的结构
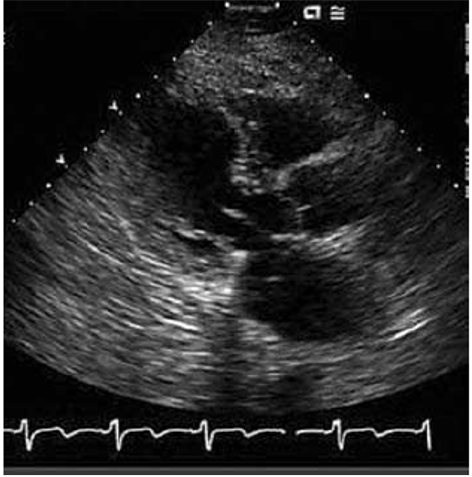
This is an end systolic frame in a patient with shortness of breath. What is the most likely diagnosis?
这是呼吸急促患者的收缩末期画面。最有可能的诊断是什么?
![]()
The left ventricle is dilated, the pumping function is poor.
Dilated cardiomypathy ethiology were still unsure cause we have to do further investigations
We can see spontaneous contrast almost in the left venture which suggests a high risk of lv thrombusThis patient is likely to have:
该患者可能患有:
![]()
可以看到胸骨旁左室长轴切面,可以看到左心室向心性肥厚。杂音会因为做 Valsalva 动作,比如下蹲,而导致杂音变响亮。
The cause of heart failure in this 30-year old man is likely to be
这名 30 岁男子心力衰竭的原因很可能是
![]()
可以看到二尖瓣反流至少呈中到重度。可以使用对比剂让图想看清晰,还可以看到左室肌小梁,这是左室致密化不全密的特征。
有时候超声检查不是很明确,可以借助其他的成像手段,比如心脏磁共振,来进行辅助诊断。

# Case Study
62 Year old Female
Rheumatic Heart Disease
Atrial Fibrillation
Chronic Kidney Disease
Tissue MVR + TV repair and LAA Ligation October 2020
On Apixaban 2.5 mg BD
62 岁的一个女性,有风湿性心脏病,房颤以及慢性肾脏疾病,2020.10 做过二尖瓣置换、三尖瓣修复和左心耳封堵,服用阿哌沙班
6 months later
Severe COVID-19 infection with Severe Pneumonia-April 2021
Hospitalised for 15 days
Kept on Apixaban
Post discharge: Significant SOBOE and Orthopnoea
Recurrent ER visits-Post COVID Sequele were blamed
六个月之后,2021.04,由于新冠感染,导致重度肺炎。住院 15 天,药物是在持续使用。
出院后出现明显的劳累性呼吸困难、端坐呼吸的一个情况。因为有新冠肺炎后遗症反复急诊就诊
Next ER admission
Pulmonary oedema
Tachypnoeic, Hypoxic with bilateral crepitation
Bilateral pitting oedema
Normal Heart Sounds
Afebrile
再次急诊入院,可以看到肺水肿,呼吸急促,缺氧,双侧凹陷性水肿,正常心音,不发烧
Labs
Anaemia (Hb=8.0)
Severe Thrombocytopaenia (Plts 60)
Normal WBC
eGFR 25 (stable)
Echo Now
左房可见明显扩张,考虑是因为该患者原来有二尖瓣狭窄和房颤病史。彩色多普勒没有看到明显的二尖瓣反流。仔细观察瓣叶,有明显的增厚和运动受限。连续多普勒频谱可以看到最大血流速度和平均跨瓣压差明显升高。
Echocardiogram TTE POST OP
术后即刻,置换的二尖瓣活动度非常好,没有明显的二尖瓣反流。连续多普勒的频谱图描绘,最大速度小于 2m/s,对于置换的人工瓣膜,这个值是合理的。
根据患者前后的超声心动图改变,以及现在患者呈现一个心衰的表现,接下来要进行哪些诊断或者治疗呢?
考虑到患者心衰的临床表现,肯定要进行抗心衰的药物治疗。
超声心电图的表现,要鉴别是赘生物还是血栓形成。
患者进行了多次血液培养,在等待结果的时候,因为不能排除到底是赘生物还是血栓形成,所以要对这两个病因进行治疗,包括广谱抗生素的使用,以及抗抗栓药物的治疗。
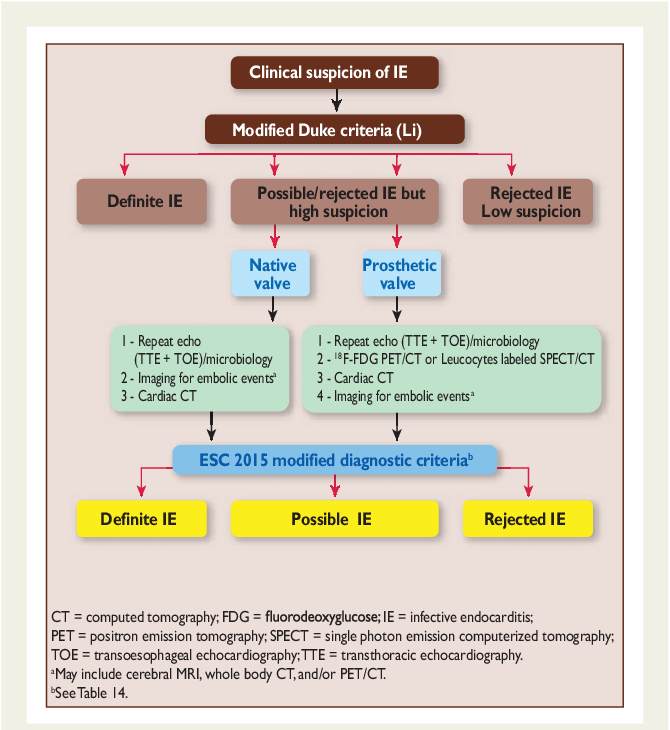
对于感染性心内膜炎,特别是对人工瓣膜植入后发生的,可以使用改良版的 Duke 标准,借助其他的成像手段,包括经食管超声心动图、 pet CT 以及心脏 CT 等来进行进一步的诊断。
三维超声心动图可以看到瓣环本身的状况是很好的。仅仅是人工瓣叶受到累及,呈现非常高跨瓣压差,没有明显的二尖瓣反流。
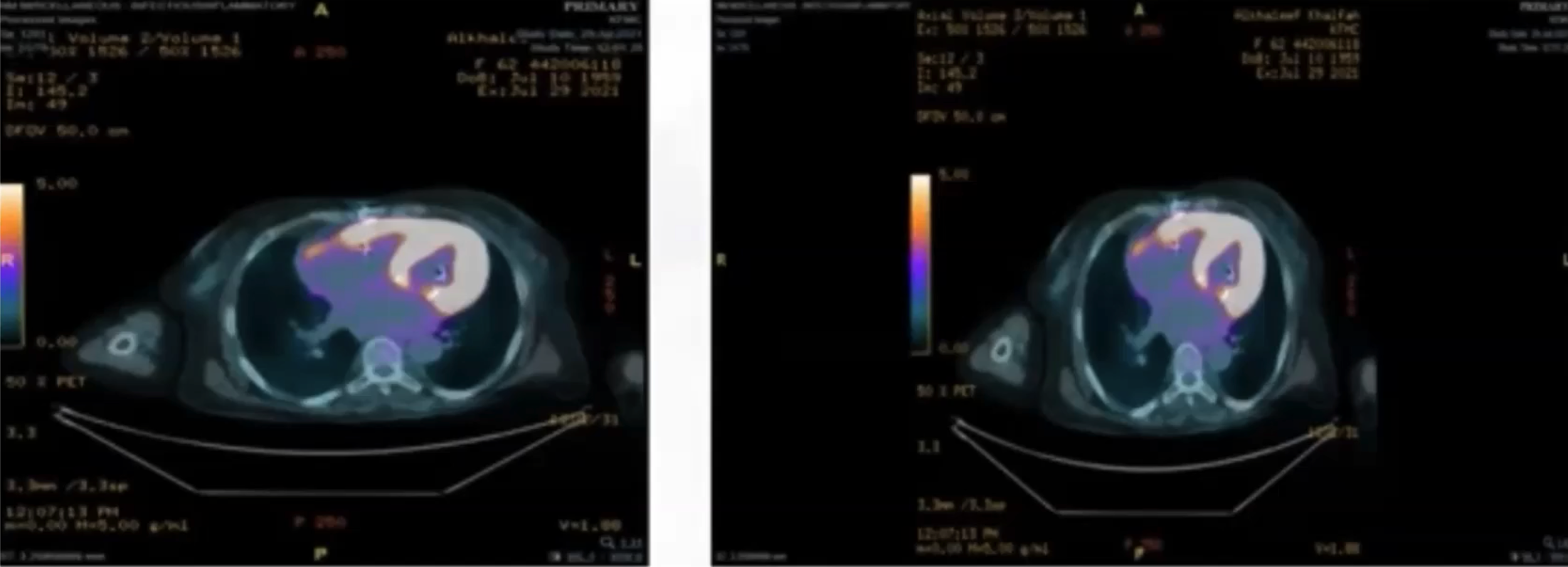
血液培养的结果呈阴性以及 pet CT 并没有提示赘生物表现。基本可以排除感染性心内膜炎的诊断。
# Mitral and Tricuspid Valve Quiz
In which view are the A2/P2 scallops visible?
在哪个切面中可以看到 A2/P2?
In which view are the P1/P3 scallops visible?
在哪个切面中可以看到 P1/P3?
Which of the following statements are true?
以下哪项陈述是正确的?
![]()
![]()
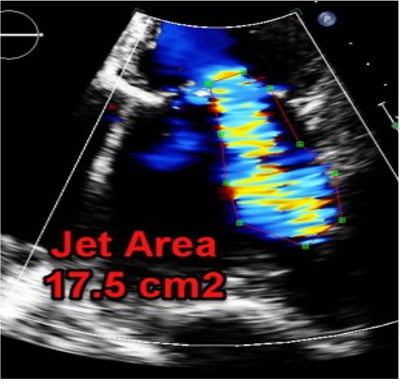
How severe is the MR?
![]()
![]()
What is the regurgitant volume?
![]()
![]()
![]()
![]()
What is the regurgitant fraction?
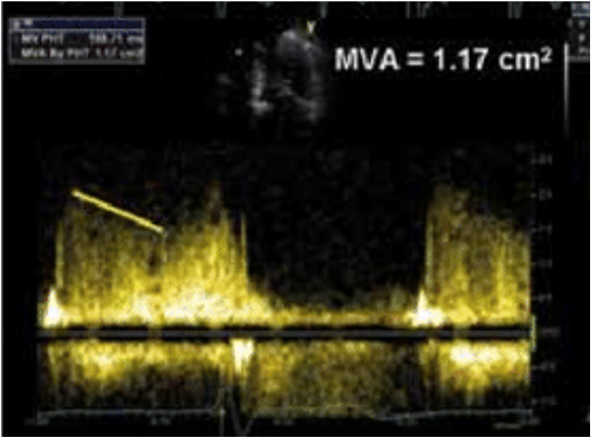
How severe is this patients mitral stenosis? (PHT = 188ms)
![]()
How severe is this patients mitral stenosis?
![]()
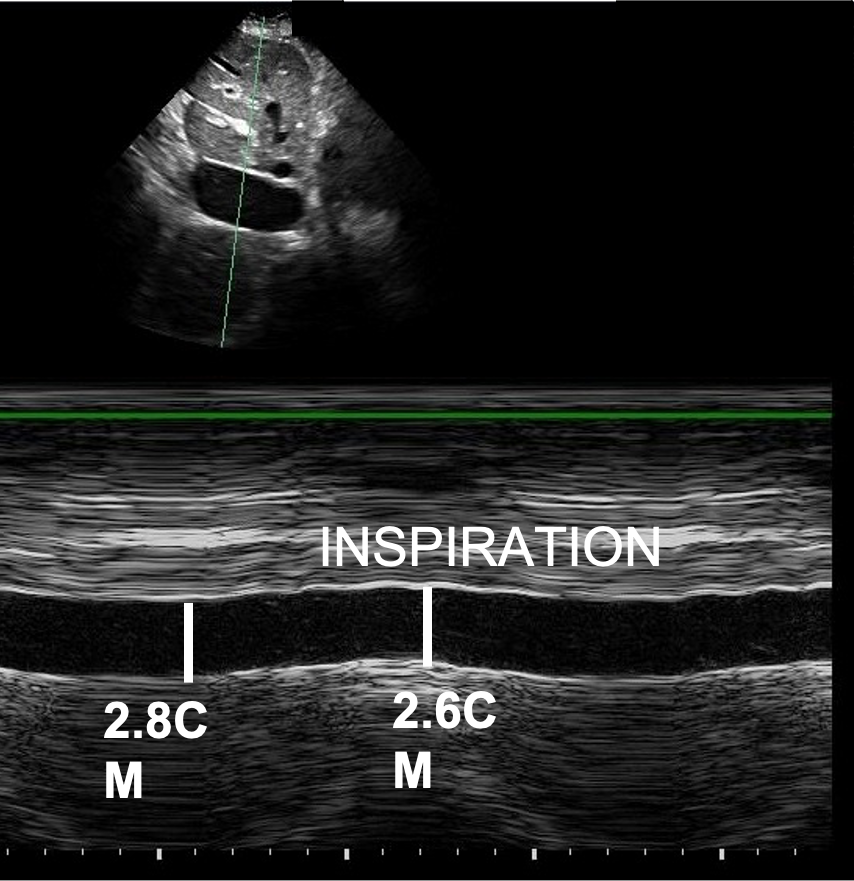
You are asked to perform an echocardiogram on a 25-year-old male who is breathless. His TR Vmax is 4m/s. His IVC is 1.2cm with complete collapse on inspiration. What is his PASP?
You perform an echocardiogram on a 62-year-old man. You find moderate pulmonary regurgitation with a peak velocity of 4.2m/s and end-diastolic peak velocity of 3m/s. The IVC is dilated at 2.6cm and collapses <50%. Which of these statements are true?
What is the severity of the tricuspid regurgitation here?
![]()
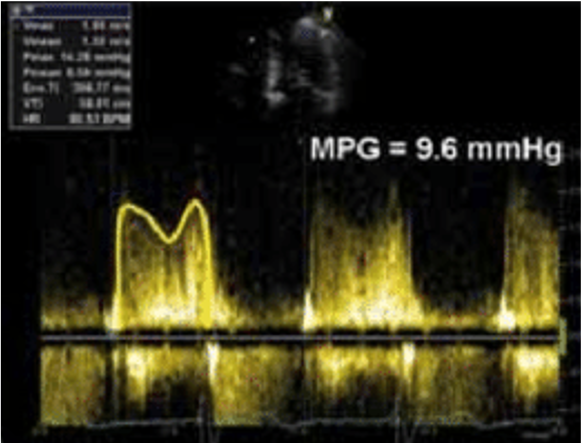
A 48-year-old male presents with peripheral oedema. A bedside echo shows a tricuspid MPG of 7mmHg. How severe is the stenosis?
A 49-year-old male presents with breathlessness. A bedside echocardiogram is performed which shows tricuspid regurgitation with VC 0.8cm, PISA radius 1.01cm. How severe is the TR?
A 49-year-old male presents with chest pain and new inferior ST changes. A bedside echocardiogram is performed which shows new mitral regurgitation with VC 0.8cm, PISA 1.1cm. How severe is the MR?
A 53-year-old female presents with breathlessness for the last 6 weeks. She had no new ECG changes but her bedside echocardiogram shows an EROA of 0.5cm2 and regurgitant fraction of 62%. How severe is the MR?
How severe is this patient’s MR?
![]()
![]()

# A Clinical Case
35-year-old male
Background: Diabetes mellitus
Medications: Metformin
Presents with episode of chest pain which lasted 2 hours
Normal chest radiograph
ECG shows non-specific ST changes
Troponin is 56 (normal 0-40).
You are asked to perform an echocardiogram.




The right atrial pressure is:
The right ventricle is:
Visually the RV systolic function is:
By colour doppler, the patient has:
The TR max pressure gradient is:
The pulmonary artery systolic pressure is:
The left ventricle is:
The PISA surface area is:
The EROA is:
The MR is:
# Echocardiography in Valve Disease - Group Test
Which two of the following statements are incorrect?
A 62-year-old man with history of long standing HTN was referred for TTE examination by a primary care provider who noticed new systolic murmur III/VI at the apex radiating to left axilla. Which of the following findings is not consistent with echocardiographic diagnosis of severe Mitral Regurgitation (MR)?
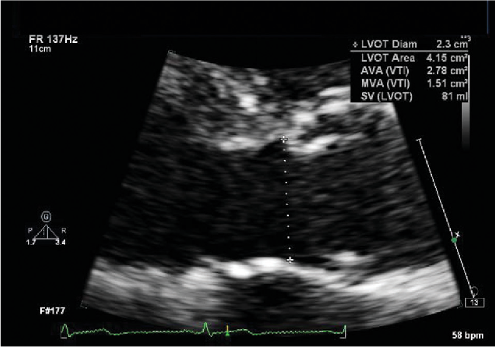
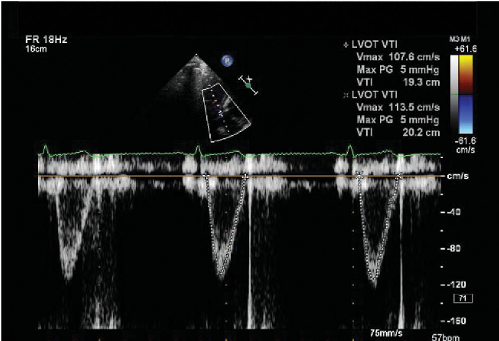
An 81-year-old man was diagnosed with severe AS by clinical examination and referred for TTE. On the TTE examination, the Left Ventricular Outflow Tract (LVOT) diameter was 2.0 cm, LVOT time velocity integral (TVI ) was 20 cm and Aortic Valve TVI was 84 cm. What is the calculated Aortic Valve Area (AVA)?
A 58-year-old man with congenital bicuspid aortic valve, complicated by moderate AS, AVA=1.1 cm², moderate Aortic Regurgitation (AR), and LVEF=60% by TTE, underwent right and left heart catheterisation. Cardiac output was measured using Fick equation and AVA was calculated. {.quiz}
If one has to predict, what was his AVA measured by invasive catheterisation?What structure is seen? (1 point) Describe the abnormalities (3 points)
![]()
Aortic valve Stenosis
Poor leaflet mobility; thickening;calcificationA 45-year-old man is diagnosed with mitral stenosis. His MVA is estimated by PHT at 1.5 cm². The patient also has bicuspid aortic and severe AR.
Which of the following statements is correct?
Describe the abnormalities (4 abnormalities)
What is the estimated severity of the disease in the valve seen?
![]()
AS, MVR, Large LA, Moderate AS
What is the Dimensionless index (velocity ratio)?
What is the grade of severity of the aortic stenosis?
This is high gradient low flow aortic stenosis (HG/LF)- true or false?![]()
![]()
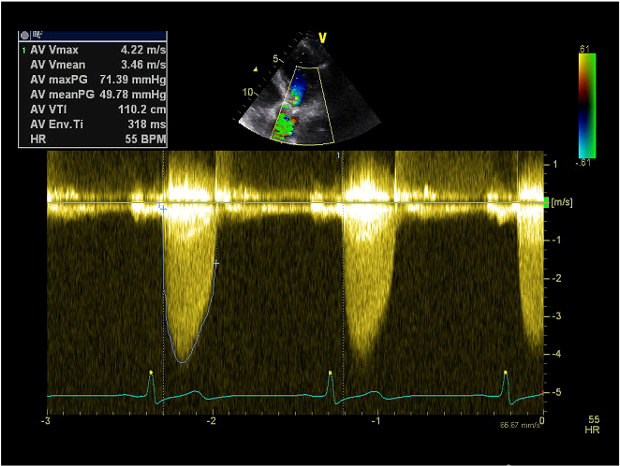
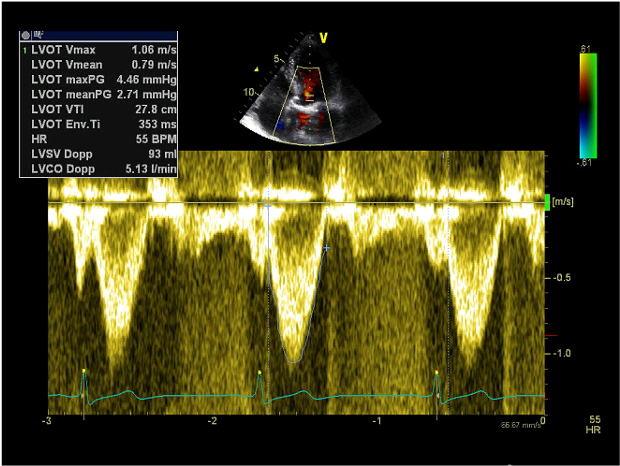
27.8/110.2, Severe, False- mean gradient > 40
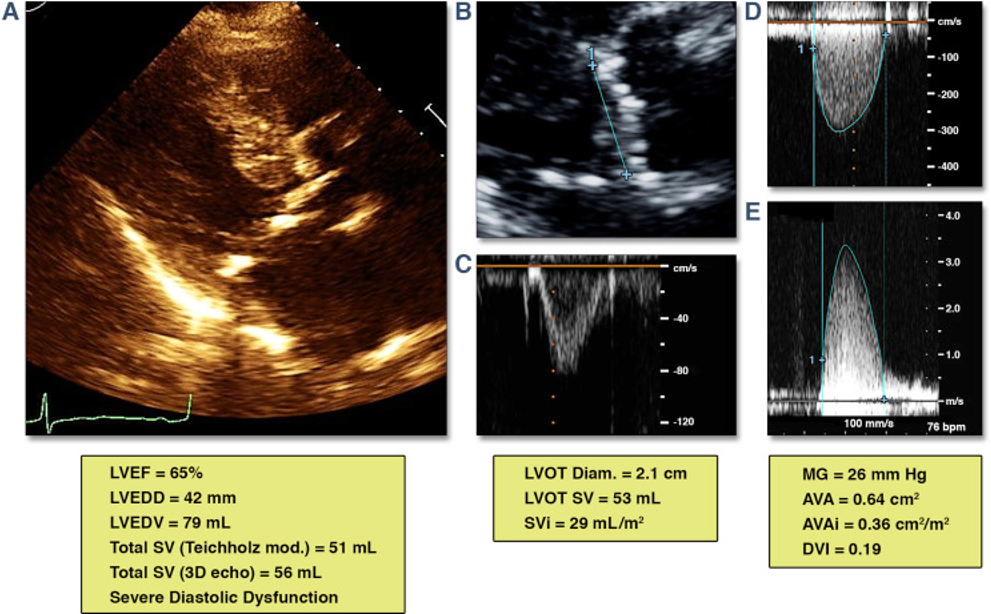
Describe the abnormalities on this echocardiogram.
How severe is this Aortic Stenosis? How would you would describe this haemodynamic state?
What further echocardiographic measurement would you suggest?![]()
![]()
Poor global LV, LA dilatation, restricted Aortic valve leaflets
Unable to be sure
Note LG/LF
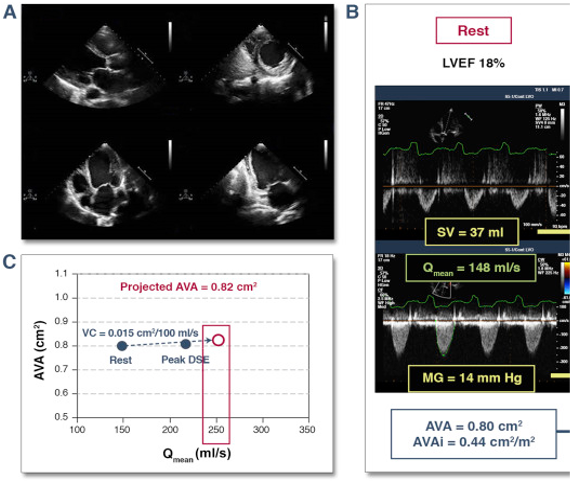
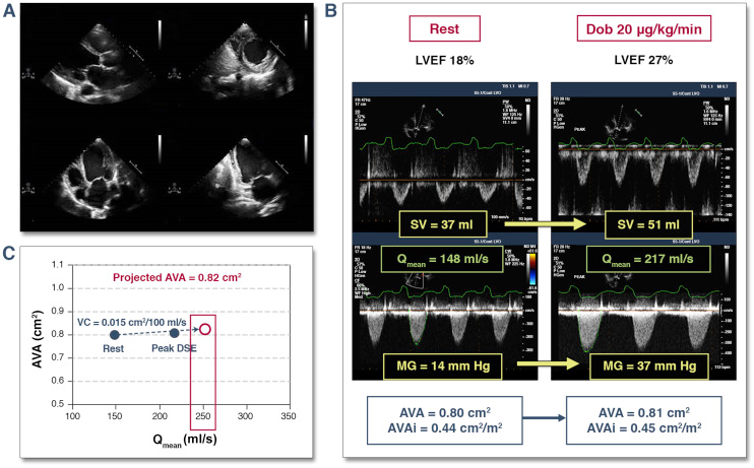
Either DSE Or CT calciumThe data from the Dobutamine study is shown. Answer true or false.
![]()
What condition is shown? {.quiz .essay}
![3rpeECWKRLVZcsU]()
Paradoxical low flow low gradient AS
What is the main abnormality seen?
What are the possible underlying aetiologies (causes)?
What is the likely severity of the haemodynamic abnormality seen?![]()
![]()
Dilated aortic root without effacement and aortic regurgitation
Hypertension, degenerative. Also consider connective tissue disease
Likely mildIn a typical patient with paradoxical LF-LG AS, select the true statements.
What is the valvular abnormality?
What is the likely cause?
How severe is the haemodynamic disturbance?![]()
![]()
Aortic valve vegetation
Endocarditis
Probably severeContinuation for Question 14:
What other measurement could you make to help quantification of the severity?
![]()
Diastolic flow reversal in the proximal descending aorta from the suprasternal view using PW doppler
A 66-year-old man who underwent AVR with a bileaflet St Jude mechanical valve 5 years ago had TTE, which was ordered due to one month worsening of SOB and DOE. Five days prior of the TTE examination, he ran out of his warfarin, INR = 3.5 on the day of TTE.
LVOT V1 = 1.6 m/sec, and AV V2 velocity 4.8 m/sec. No significant AR was note. His TTE report from 1 year ago indicated that LVOT V1 was 0.8 m/sec and AV velocity was 2.4 m/sec. Which one of the following statements is correct?