# Learning objective
- Mitral valve Anatomy 二尖瓣解剖
- Echocardiographic visualisation of the mitral valve 二尖瓣的超声心动图目测观
- Mechanisms of MR 二尖瓣反流的机制
- Carpentier classification of mitral regurgitation 二尖瓣反流的 Carpentier 分型
- Role of 3D echocardiography 三维超声心动图的作用
# Mitral Valve Apparatus 二尖瓣装置
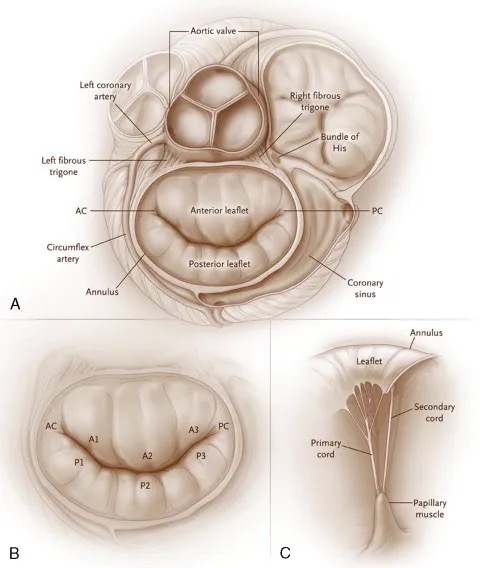
- Saddle-shaped eclipse 马鞍形结构
- Most apical points seen in apical 4 chamber
大多数瓣尖部分见于心尖四腔切面 - Most basal points seen in parasternal long axis
大多数瓣膜基底部见于胸骨旁长轴 - Annular area usually 5-11cm2
瓣环面积通常为 5-11cm2 - Posterior part is easily dilated compared to anterior part of annulus.
瓣环后部比前部更容易扩张
| 结构 | 病变 |
|---|---|
Annulus | Dilatation / calcification |
Leaflets | Prolapse, redundancy 脱垂,冗余 |
Chordae tendinae | Abnormal insertion 插入异常 |
Papillary muscles | Ischemia 缺血 |
LV free wall | Lateral displacement (ischemia, fibrosis, dilatation) |
# Visualising the Mitral Valve 二尖瓣的可视化
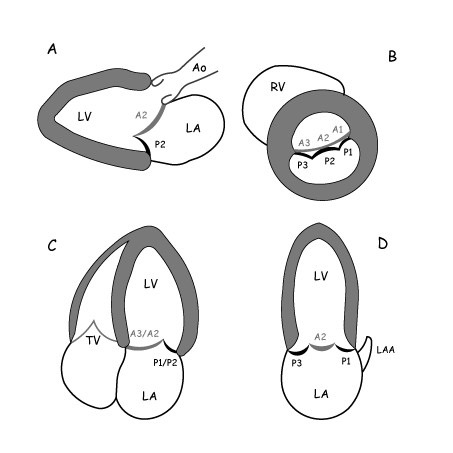
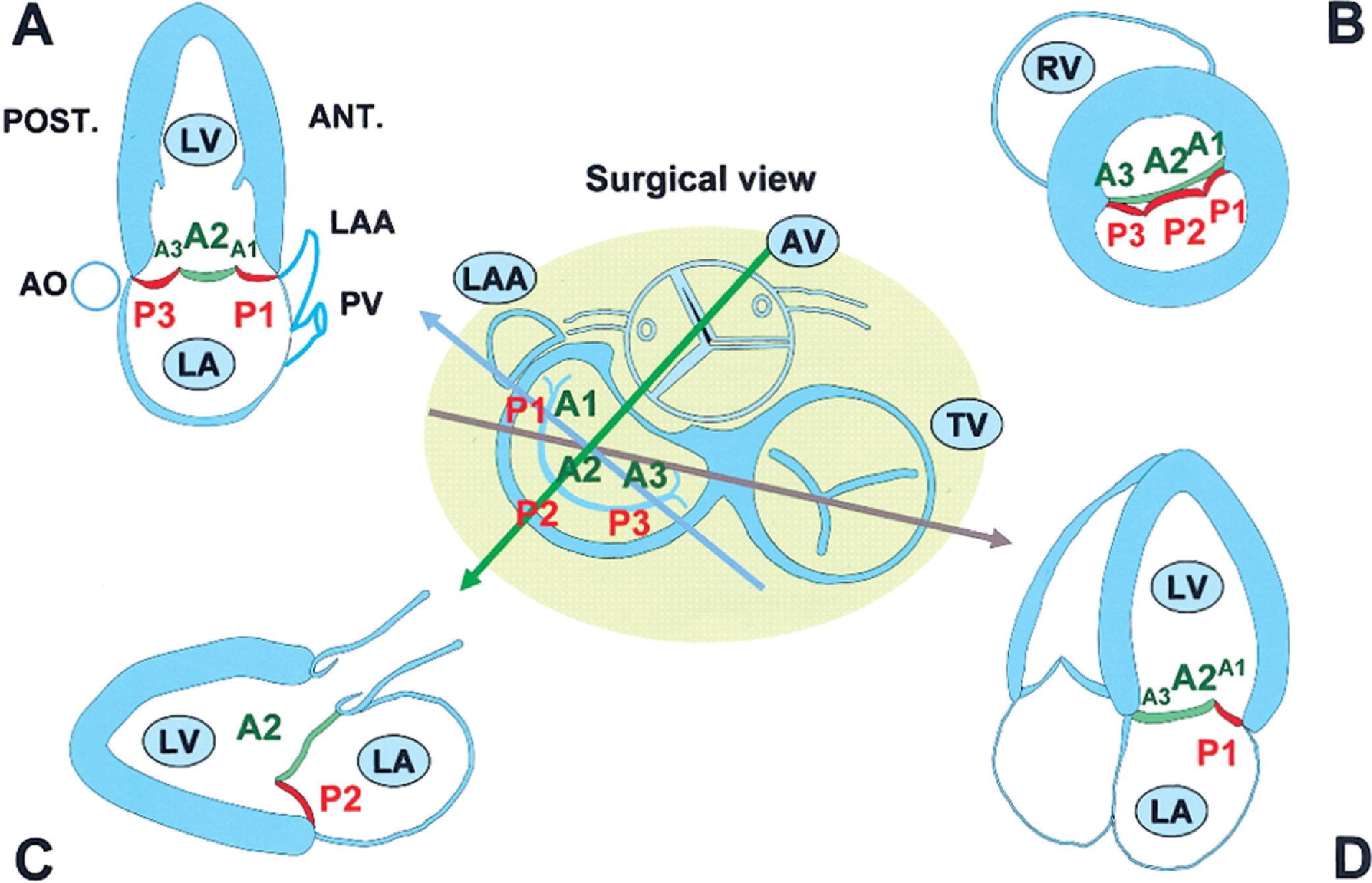





- Standardized 2D-TTE imaging planes to assess the precise localization of prolapsing or flailing segments. [1][2]
(A) PLAX: A2 / P2
(B) PSAX: A1-3 / P1-3
(C) A4C: A2-3 / P1
(D) A2C: A2 / P1 and P3
# Mechanisms of MR
- MV leaflets do not cover the annulus orifice throughout LV systole
在左室收缩期间,MV 瓣叶不能覆盖整个瓣环口- Primary MR - Leaflet pathology
原发性 MR - 瓣叶病变 - Secondary MR - LV myocardial pathology
继发性 MR - 左室心肌病变
- Primary MR - Leaflet pathology
- MR can be functionally classified based on MV leaflet pliability and motion (Carpentier Classification)
MR 可以根据二尖瓣瓣叶的柔韧性和运动进行功能分类 (Carpentier 分类) - MV leaflet malcoaptation and MR jet origin are commonly indicated by anterior (A) or posterior (P) leaflet and lateral (A1/P1), central (A2/P2) or medial (A3/P3) scallop location.
MV 瓣叶对合不良和 MR 反流束起源,通常用前 (A) 或后 (P) 瓣叶,和外侧 (A1/P1)、中央 (A2/P2) 或内侧 (A3/P3) 瓣叶位置来表示。
# Primary MR 原发性
# 病因
- Degenerative: 退行性
- Barlow’ disease 又称原发性二尖瓣脱垂、先天性二尖瓣脱垂或黏液样病变二尖瓣脱垂
- fibroelastic degeneration 纤维弹性退行性变
- Marfan's 马凡综合征,一种遗传性结缔组织疾病
- Ehlers Danlos syndrome 一种先天性结缔组织发育不全综合征
- annular calcification 瓣环钙化
- Rheumatic: Fibrosis of the chordae
风湿性:腱索纤维化 - Infective endocarditis 感染性心内膜炎
# 治疗
- Valve replacement or repair 瓣膜置换或修复
# Secondary / Functional MR 继发性
# 病因
- Ischaemic MR 缺血性
- Cardiomyopathy 心肌病
# 治疗
- May improve with heart failure therapy, resynchronisation therapy, coronary revascularisation
先行病因治疗,心力衰竭治疗、再同步化治疗、冠状动脉血管重建术可能会改善反流 - Accurate assessment of the functional anatomy is a prerequisite for successful mitral valve repair
准确评估二尖瓣功能解剖是二尖瓣修补术成功的前提
# Carpentier Classification
- Describes the mechanism of mitral valve dysfunction [3]
描述二尖瓣功能障碍的机制

# Primary MR 原发性
# Degenerative MR 退行性二尖瓣反流
Myxomatous degeneration of the leaflets
瓣叶粘液瘤样退化If part of either leaflet goes > 2mm behind the MV annulus in parasternal long axis view
如果在胸骨旁长轴切面中,任一瓣叶的一部分在二尖瓣瓣环后 > 2mmTwo main types 两种主要类型 [4]
- Fibroelastic deficiency: Focal segmental deficiency
纤维弹性缺乏:局灶性节段性缺乏 - Barlow's disease: Diffuse thickening and redundancy affecting both leaflets/chordae
巴洛氏病:弥漫性增厚和冗长,累及瓣叶 / 腱索
- Fibroelastic deficiency: Focal segmental deficiency



(A) In normal mitral valve, the coaptation (red point) occurs beyond the mitral annular plane (line);
在正常的二尖瓣中,对合 (红点) 发生在二尖瓣环平面 (线) 之外(心室面);
# Ballooning or Billowing 翻滚
(B) billowing mitral valve is observed when a part of the mitral valve body protrudes into the left atrium (arrow);
当二尖瓣瓣体的一部分突出到左心房时,观察到翻滚的二尖瓣(箭头);
- Part of the MV body protrudes in to the left atrium
部分瓣膜突入左心房,(降落伞样) - The coaptation point is preserved beyond the annular plane
对合点依旧保持在环形平面之外 - MR is usually mild in this condition
在这种情况下,MR 通常是轻度的
# Prolapse 脱垂
(C and D) Mitral valve prolapse is defined as abnormal systolic displacement of 1 (C posterior prolapse) or both leaflets into the left atrium below the annular (D bileaflet prolapse);
二尖瓣脱垂定义为一个 (C 后叶脱垂) 或两个瓣叶 (D 双叶脱垂) 收缩期异常移位,瓣体 + 瓣尖均进入左房;
- Diagnosis should be made in PLAX because the saddle shaped annulus may lead to false positives in A4C
应在 PLAX 中进行诊断,因为瓣环呈马鞍形,可能导致 A4C 下得到假阳性的结果 - Leaflet malcoaptation is greatest in mid-late systole, hence, MR occurs
瓣叶错位在收缩中晚期最严重,因此发生了反流。 - Failure to recognise that MR is not holosystolic can lead to overestimation of MR severity
如果 MR 不是全收缩期的,可能导致严重程度被高估

# Flail 连枷
(E) flail of the anterior leaflet (arrow)
前叶连枷 (箭头)
Cause
- Chord or papillary muscle rupture due to MI
心肌梗死导致的腱索或乳头肌破裂 - Myxomatous degeneration
粘液瘤样变性
- Chord or papillary muscle rupture due to MI
Echo findings
- Eccentric direction of MR jet
偏心性反流束 - Free edge of the leaflet is reversed towards the LA
瓣叶游离缘朝左心房翻转 - Posterior leaflet is most affected (70% of cases).
后叶受累最多见 (70%)
- Eccentric direction of MR jet

")
# Rheumatic MR 风湿性二尖瓣反流
- Leaflet tip thickening with restricted movement
瓣叶尖端增厚,运动受限 - Fusion of the leaflet commissures reducing orifice area - Typical doming of leaflets in diastole
瓣叶交界区融合,减少了瓣口面积 —— 舒张期瓣叶呈现典型的隆起样改变 - Fibrosis of the chordae attached to posterior leaflet is more frequent - Rigid and reduced motion of posterior leaflet in diastole
附着于后叶的腱索发生纤维化更为常见 —— 舒张期,后叶运动僵硬、减少 - Semi-open position of posterior MV leaflet throughout cardiac cycle (hence, anterior leaflet appears to prolapse)
在整个心动周期中,后叶呈半开放状态(因此,前叶看起来像有脱垂)

# Infective Endocarditis 感染性心内膜炎
- Leaflet destruction 瓣叶损坏
- Perforation 穿孔
- Deformity 畸形
- Vegetations can prevent leaflet coaptation
赘生物影响瓣叶对合




# Functional MR 功能性
- Abnormal function of normal mitral valve leaflets [5]
二尖瓣叶结构正常,而功能异常 - Due to LV dilatation +/- systolic dysfunction
由于左心室扩张 伴或不伴 收缩功能障碍 - Dilated annulus (annulus : anterior leaflet ratio > 1.3 or annulus >35mm)
瓣环扩张(瓣环:前叶比值 > 1.3 或者瓣环 > 35mm) - Apical papillary muscle displacement
乳头肌向心尖部移位 - Apical tethering of leaflets
瓣叶被牵拉向心尖部 - Leads to increased tenting area "seagull sign"
导致(灰色)瓣叶下帐篷面积增加,帐篷形态被称为 “海鸥征” - Increased mitral coaptation depth with incomplete coaptation
增加了二尖瓣对合深度,且对合不完全

- At rest, regurgitant volume depends on systolic pressure gradient across the orifice, duration of systole, and effective regurgitant orifice(ERO) dimension.
静息时,反流量取决于反流口 ERO 的收缩压差、收缩持续时间和有效反流口大小。- During exercise, systolic pressure gradient increases, duration of the systole decreases, and regurgitant volume is strictly dependent on the size of ERO.
在运动过程中,收缩压差增加,收缩持续时间减少,反流量严格取决于 ERO 的大小。- Thus, FMR varies very differently from one patient to another during exercise and no correlation is observed with resting ERO.
因此,FMR 在运动过程中因患者而异,并且与静息 ERO 没有相关性。- Rather, the tenting area enclosed between leaflets and anular plane and the coaptation distance (the distance between annulus plane and coaptation point of the leaflets) become of critical importance in predicting exercise-induced changes in ERO
相反,瓣叶和瓣环平面之间的帐篷区域和对合距离(瓣环平面和瓣叶的对合点之间的距离)对于预测运动引起的 ERO 变化至关重要
LV Remodelling and MV Distortion Results in imbalance between the tethering forces and closing forces [6]
LV 重塑和 MV 变形,导致束缚力和闭合力之间的不平衡- Asymmetrical pattern (95%): Ischaemic
不对称型 (95%):缺血 - Symmetrical pattern (5%): Non-ischaemic cardiomyopathy
对称型(5%):非缺血性心肌病
- Asymmetrical pattern (95%): Ischaemic
When reviewing the aetiology of functional MR assess if it is regional LV dysfunction or global LV dysfunction
当回顾功能性 MR 的病因学时,需要评估是局部左心功能不全还是整体左心功能不全- Regional LV dysfunction is secondary to inferior MI - Posteriorly directed eccentric MR
局部节段性左室功能障碍继发于下壁心肌梗死 —— 后向偏心性反流 - Global LV dysfunction is due to non-ischaemic cardiomyopathy, large anterior or multiple regjon MI - Central MR.
整体左心功能不全是由非缺血性心肌病、广泛前壁或多发性心肌梗死所致的 —— 呈中央性反流
- Regional LV dysfunction is secondary to inferior MI - Posteriorly directed eccentric MR


- Seagull Sign 海鸥征
- Apical displacement of papillary muscles and dilated LV with 'spherical shape'
当左心室扩张呈 “球形”,乳头肌会向心尖移位 - Leads to apical tethering of mitral leaflets
导致二尖瓣叶也向心尖栓系 - Traction on the anterior MVL by the secondary chordae results in the seagull sign.
次级腱索在前叶上的牵引会导致海鸥征出现
- Apical displacement of papillary muscles and dilated LV with 'spherical shape'


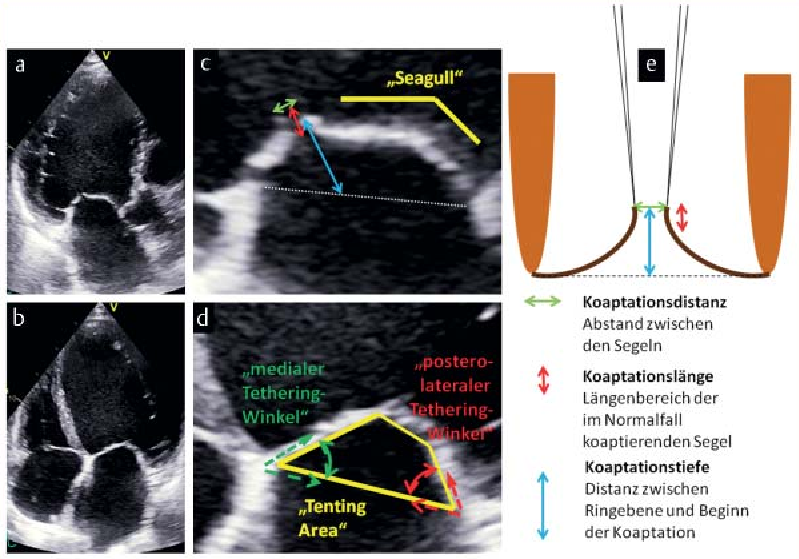
- Documentation of special morphological parameters for characterizing mitral valve deformation: [7]
二尖瓣变形特征的特殊形态学参数记录:- 2D apical long axis view a and 2D apical 4-chamber view b during systole showing the mitral valve of a patient with functional mitral valve regurgitation.
收缩期 2D 心尖长轴切面 a 和 2D 心尖四腔切面 b,显示患有功能性二尖瓣反流的患者的二尖瓣。 - ZOOM images of the particular sections of the mitral valve with the individual deformation parameters drawn in c, d.
二尖瓣特定部分的 ZOOM 图像,单个变形参数绘制在 c,d 中。 - Schematic drawing for explaining the parameters coaptation distance, coaptation length and coaptation depth e.
说明对合距离、对合长度和对合深度等参数的示意图。
- 2D apical long axis view a and 2D apical 4-chamber view b during systole showing the mitral valve of a patient with functional mitral valve regurgitation.
# Nonischemic Cardiomyopathy
- Morphologic Changes in Heart Failure 心力衰竭的形态学变化
- Papillary muscles are displaced apically and laterally [8]
乳头肌在向心尖和侧壁移位
- Papillary muscles are displaced apically and laterally [8]

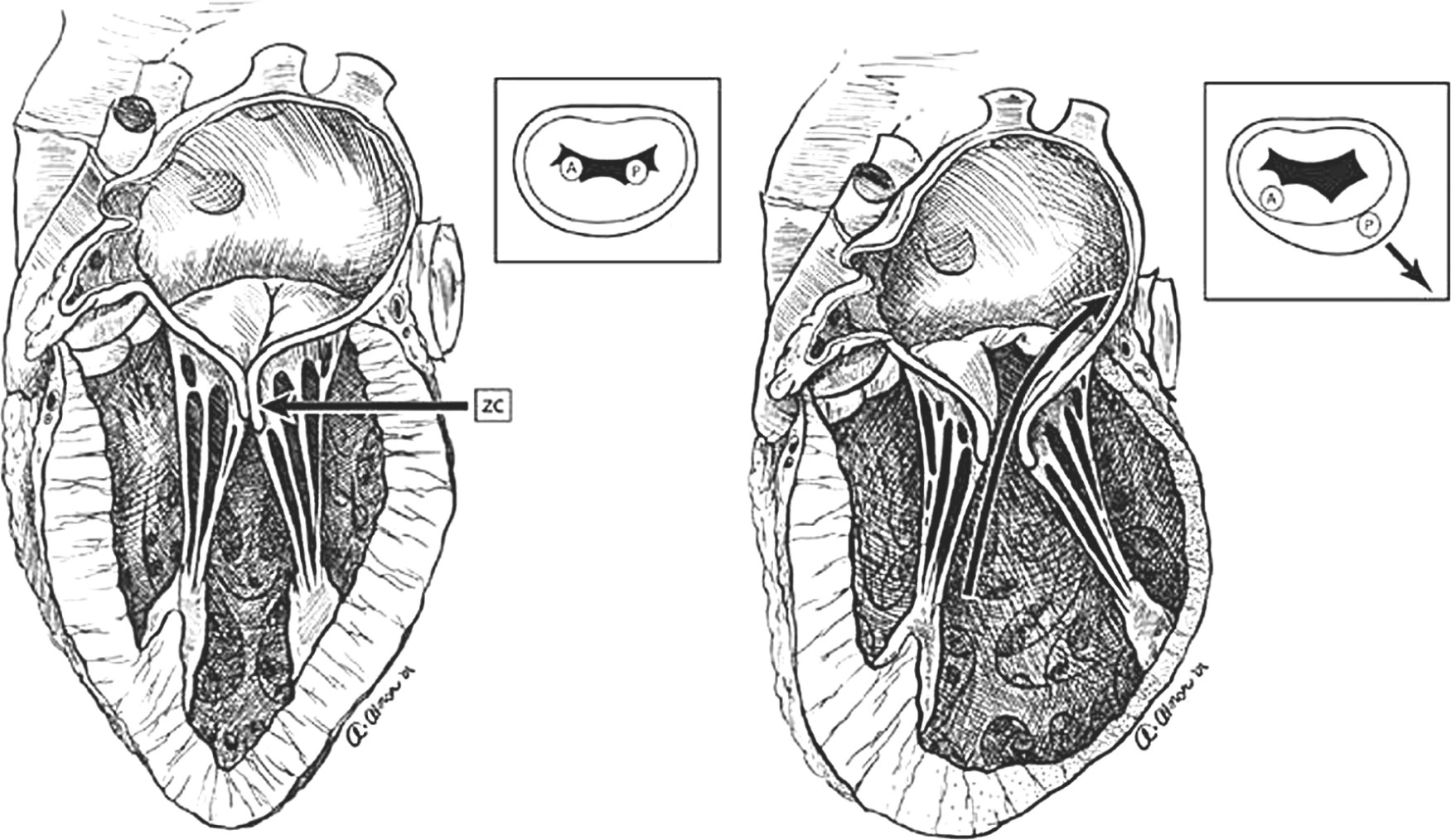
- Shown on the left is the normal mitral apparatus and its effective zone of coaptation (ZC), while changes that occur in heart failure are shown on the right.
左侧显示正常的二尖瓣装置及其有效对合区 (ZC),而右侧显示心力衰竭发生时的变化。 - Theses alterations include myocardial thinning and dilatation, blunting of the aorto-mitral angle, widening of the interpapillary distance, increased leaflet tethering, and decreased leaflet-closing forces.
这些改变包括心肌变薄和扩张,主动脉 - 二尖瓣角变钝,毛细血管间距离变宽,瓣叶栓系增加,瓣叶闭合力降低。 - This leads to altered force vectors on the papillary muscles (see insets).
这导致乳头肌上的力向量发生改变(见右上角插图)。 - These morphologic changes combine to result in loss of the zone of coaptation and central mitral regurgitation.
这些形态变化共同导致二尖瓣对合区的丧失和中央性二尖瓣反流。
# Ischaemic MR 缺血性二尖瓣反流
Moderate to severe MR due to a myocardial infarction or resulting LV remodeling in the absence of primary, preexisting leaflet or chordal pathology.
在没有原发性、先前存在的瓣叶或腱索病变的情况下,由于心肌梗死或继发的左室重塑导致的中度至重度二尖瓣反流。Causes: 病因
- Dislocation of papillary muscles
乳头肌脱位 - Increased tenting length and area
增加帐篷长度和面积 - Antero-posterior dilatation of the MV annulus
二尖瓣瓣环前后扩张 - Kinetics of MV annulus during cardiac cycle
心动周期中二尖瓣瓣环的动力学 - Intraventricular dyssynchrony
心室内不同步 - Atrioventricular dyssynchrony
房室不同步
- Dislocation of papillary muscles
Generally, one papillary muscle involved
通常,一个乳头肌受累Usually due to inferolateral wall hypokinesia (RCA/ LCx)
通常由于下外侧壁运动障碍(右冠或回旋支)Posteriorly directed MR jet due to abnormal coaptation.
由于对合异常,反流束向后
- In ischemic cardiomyopathy, changes within the left ventricle (LV) may be asymmetric and still lead to functional mitral regurgitation.
在缺血性心肌病中,左心室(LV)内的变化可能不对称,仍然会导致功能性二尖瓣反流。 - With ischemic damage and thinning of the ventricular wall, there is lateral tethering, displacement of the papillary muscle, and loss of the zone of coaptation (ZC), resulting in an eccentric jet of mitral regurgitation.
随着缺血损伤和心室壁变薄,出现横向束缚、乳头肌位移和对合区(ZC)的丧失,导致二尖瓣反流的偏心反流束。 - This illustrates the concept that ischemic mitral regurgitation results from “lateral wall dysfunction” that, if left untreated, will progress to global LV dysfunction and severe heart failure.
这说明了一个概念,即缺血性二尖瓣反流是由 “侧壁功能障碍” 引起的,如果不加以治疗,将发展为整个左室功能障碍和严重心力衰竭。

- RCA occlusion with residual inferolateral aneurysm
右冠状动脉闭塞,下外侧壁基底段可见室壁瘤,中段呈无运动,彩色多普勒可见后向反流束

- RCA occlusion with PM papillary muscle rupture
右冠状动脉闭塞伴后内侧乳头肌破裂
# Role of 3D
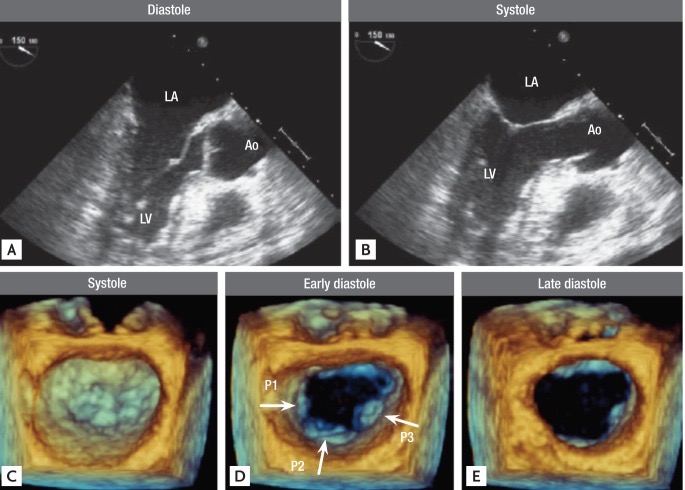
Normal mitral valve imaged by 2-dimensional (D) echo (A, a long axis view in diastole; B, in systole) and real-time 3D transesophageal echocardiography (C, a view from the left atrium in systole; D, in eerily diastole; E, in late diastole). Arrows indicate each leaflet: lateral P1, middle P2, and medial P3. Ao, aorta; LA, left atrium; LV, left ventricle.
正常二尖瓣通过二维(D)超声心动图(A,舒张期长轴视图;B,收缩期)和实时三维经食管超声心动图成像(C,收缩期左心房视图;D,舒张异常;E,舒张晚期)。箭头指示每个小叶:外侧 P1、中间 P2 和内侧 P3。
Minardi, G. et al. Preoperative scallop-by-scallop assessment of mitral prolapse using 2D-transthoracic echocardiography. Cardiovasc Ultrasound 8, 1–9 (2010). ↩︎
Monin, J.-L. et al. Functional Assessment of Mitral Regurgitation by Transthoracic Echocardiography Using Standardized Imaging Planes. Journal of the American College of Cardiology 46, 302–309 (2005). ↩︎
Zoghbi, W. A. et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr 30, 303–371 (2017). ↩︎
Lancellotti, P. et al. Recommendations for the echocardiographic assessment of native valvular regurgitation: an executive summary from the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 14, 611–644 (2013). ↩︎
Bigi, R., Cortigiani, L., Bovenzi, F. & Fiorentini, C. Assessing functional mitral regurgitation with exercise echocardiography: rationale and clinical applications. Cardiovascular Ultrasound 7, 57 (2009). ↩︎
Lancellotti, P., Zamorano, J.-L. & Vannan, M. A. Imaging challenges in secondary mitral regurgitation: unsolved issues and perspectives. Circ Cardiovasc Imaging 7, 735–746 (2014). ↩︎
Hagendorff, A., Stoebe, S., Tarr, A., & Pfeiffer, D. (2015). Standardized transthoracic echocardiography in patients with primary and secondary mitral valve regurgitation. Ultraschall in der Medizin, 36 1, 10-34 . ↩︎
Suzuki, Y., Spoor, M.T., Bolling, S.F. (2008). Mitral Valve Repair. In: Raman, J. (eds) Management of Heart Failure. Springer, London. ↩︎